Most system implementations don’t fail outright. They stall. Timelines stretch. Decisions slow. Teams burn out managing change alongside daily operations.
Where Execution Breaks Down
Common risk points include:
Diffuse accountability across teams
Competing priorities and limited capacity
Vendor-led timelines disconnected from operations
Lack of adoption ownership after launch
Why This Matters
When execution falters:
ROI is delayed or lost
Teams revert to workarounds
Leadership confidence erodes
ProspHire Perspective
ProspHire mitigates execution risk by providing:
Clear ownership and governance
Disciplined delivery management
Alignment across IT, operations and leadership
Execution isn’t a phase; it’s the work. When system implementations fall short, the root cause is rarely technology; it’s execution under pressure. Clear ownership, disciplined delivery and operational alignment are what prevent delays, burnout and stalled adoption. Addressing execution risk early is what separates stable implementations from ones that struggle to deliver value.
The Challenge: You Can’t Improve What You Don’t Understand
In today’s Stars environment, health plans are expected to deliver stronger performance while managing varying contract maturity levels, operational capabilities, geographic variability and diverse member populations. At the same time, regulators continue to refine the program, most recently theproposed CY 2027 rule, adding complexity and volatility to an already high-stakes system.
As pressure mounts, plans must do more than improve outcomes. They must understand whether their contracts are positioned to perform, sustain and scale success.
Without a clear baseline, benchmarking or contract readiness evaluation, plans risk investing in the wrong strategies, duplicating effort or missing meaningful opportunities for improvement.
What High-Performing Plans Are Doing Differently
Leading organizations are pausing before they push forward. Rather than spreading resources evenly across contracts or chasing isolated measure improvements, they begin by gaining a clear picture of where they stand.
This disciplined approach enables targeted improvement, reduces waste and focuses effort where it will generate the greatest return.
Three Priorities for Contract Benchmarking and Readiness
Contract-Level Benchmarking: Measure competitive standing by contract to identify improvement opportunities, risk exposure and of performance leverage.
Operational Readiness Assessment: Evaluate the core health plan capabilities that drive Stars performance, including analytics, governance, provider engagement, member experience strategies and vendor accountability.
Targeted Investment and Strategy Alignment: Use assessment insights to direct resources toward contracts with the strongest opportunity for sustainable performance improvement.
Our Perspective
At ProspHire, we believe the strongest Stars strategies begin with precision, knowing exactly where you are before deciding where to go next. Through Contract insight, operational assessment and focused prioritization, create the clarity plans need to aim higher with confidence and measurable impact.
Measure. Benchmark. Improve with Purpose.
Stars improvement begins with understanding. Let’s redefine how you benchmark performance, assess readiness and elevate contract performance outcomes with a strategy built on clarity, focus and execution.
Connect with ProspHire to learn how a contract-level Stars assessment can position your plan for sustainable success.
The next phase of dental practice evolution will not be defined by the systems organizations select but by how effectively they execute.
As DSOs and DPOs continue to modernize technology, centralize operations and standardize workflows, the organizations that succeed in 2026 will be those that connect strategy to frontline delivery across their partner and affiliate practices.
Systems Integration Advisory
As DSO/DPO leaders and equity owners shift from legacy systems to fully integrated imaging, clinical and revenue management platforms, demand is rising for partners who can manage not only system selection but execution across data, people and workflows.
This includes:
Data migration and system configuration
Staff training and adoption
ROI protection during and after go-live
ProspHire Perspective:
ProspHire leads end-to-end Dental Practice Management System (DPMS) conversions using a proven framework designed to strengthen operations while minimizing risk.
Supported 160+ general and specialty practices across four national dental organizations.
Experience across general dentistry, oral surgery, pediatric, endodontics, periodontics and orthodontics.
Practices maintain or exceed pre-conversion scheduling performance through optimized templates and new workflow standardizations.
Onsite delivery supported onsite by clinical, IT and practice management specialists who understand both general and specialty dentistry.
Strategic advisory combined with delivery services enables practices to remain fully operational during go-live, improving ROI and reducing risk.
DPMS Conversion and Technology Consolidation
In 2026, successful implementations will be defined equally by the technology chosen and by the quality of training, change management and adoption. Partners who connect strategy to frontline execution will be essential.
ProspHire Perspective:
Standardized conversion methodology with consistent documentation and “repeatable processes”.
“At-the-elbow” onsite training to reduce disruption and staff turnover.
Poven ability to execute at scale.
Example:
We successfully converted nine practices in one weekend across three states, deploying a coordinated teamof 26 project management, IT, clinical and revenue cycle specialists supported by virtual command centers.
Our approach protects production, preserves schedules and accelerates value realization from technology investments.
Revenue Cycle Transformation
Revenue leakage is one of the highest-risk areas during transformation but also one of the greatest opportunities for recovery, stability and long-term savings.
Inefficient billing, missed claims, poor data integrity and weak reporting increases the demand for revenue cycle transformation services during conversion events and centralization activities.
ProspHire Perspective:
DPMS conversions paired with centralization and new automated revenue cycle vendors significantly increase risk without proper configuration and workflow oversight.
Accurate plan builds, fee schedules and practice setup are essential to prevent rejected claims. inaccurate payments and incorrect treatment plan presentations.
Delaying revenue cycle integration creates costly rework and revenue disruption.
ProspHire aligns revenue cycle workflows, centralization and vendor integration before or during DPMS conversions to protect cash flow and operational stability.
Merger and Acquisition Readiness
Clean data, standardized workflows, compliance readiness and efficient technology are increasingly central to valuation for DSOs pursuing growth or private equity investment.
ProspHire Perspective:
Supported national DSOs and DPOs in converting multi-specialty practices across multiple DPMS platforms.
What began as a seasonal campaign became something more intentional: a focused, twelve-day reflection on the pressures reshaping healthcare and the execution required to navigate them.
At a time when policy shifts, operational strain and digital transformation are accelerating simultaneously, healthcare leaders don’t need more noise. They need clarity. They need perspective. And most importantly, they need practical pathways forward.
Our “12 Days of Care & Cheer” insight series was designed to do exactly that: spotlight the realities facing health plans and providers while reinforcing the discipline, structure and follow-through required to turn strategy into results.
Twelve days of focused industry reflection created more than visibility, it created momentum. Each topic reflected real challenges facing healthcare organizations, from operational strain to digital transformation to patient access. The content didn’t just explore trends; it highlighted pain points and connected them directly to capabilities designed to alleviate friction, reduce inefficiencies and strengthen performance across the care continuum.
Turning Strategy into Stronger Outcomes
The work behind these conversations reflects a broader commitment to helping healthcare organizations achieve better health outcomes. By addressing inefficiencies, strengthening systems and supporting adoption at every level, organizations are better equipped to enhance care delivery, improve patient experiences and drive meaningful, measurable results.
At the center of every challenge and every solution are:
Patients seeking better experiences
Providers delivering care under pressure
Leaders responsible for long-term stability and innovation.
Progress in healthcare is not defined solely by systems or strategy, but by how effectively those systems empower the individuals behind them. When operational excellence and people-first execution align, meaningful and lasting improvement becomes possible.
On November 25, 2025, CMS released the Contract Year (CY) 2027 Medicare Advantage and Part D Proposed Rule, a 400+ page regulation that reaches into nearly every aspect of MA and Part D operations.
Paired with the RFI on the future of Medicare Advantage, this rule marks a true turning point in the Medicare Advantage program. We’ve been talking a lot recently about the Medicare Advantage Reset and the need for plans to take a hard look at their models for success and now CMS has acted. Through the Proposed Rule, CMS is looking to simplify the program by reducing administrative burdens for marketing oversight, while also setting the stage for bigger shifts in risk adjustment, Stars & quality bonus payments and special needs plans. Plans need to take this moment seriously and recognize we’ve moved beyond business as usual. We’re now in the next era of Medicare Advantage.
Executive Summary: Four Big Themes for Plans
From a plan and operator perspective, four primary themes stood out to us in this proposed rule and related RFIs:
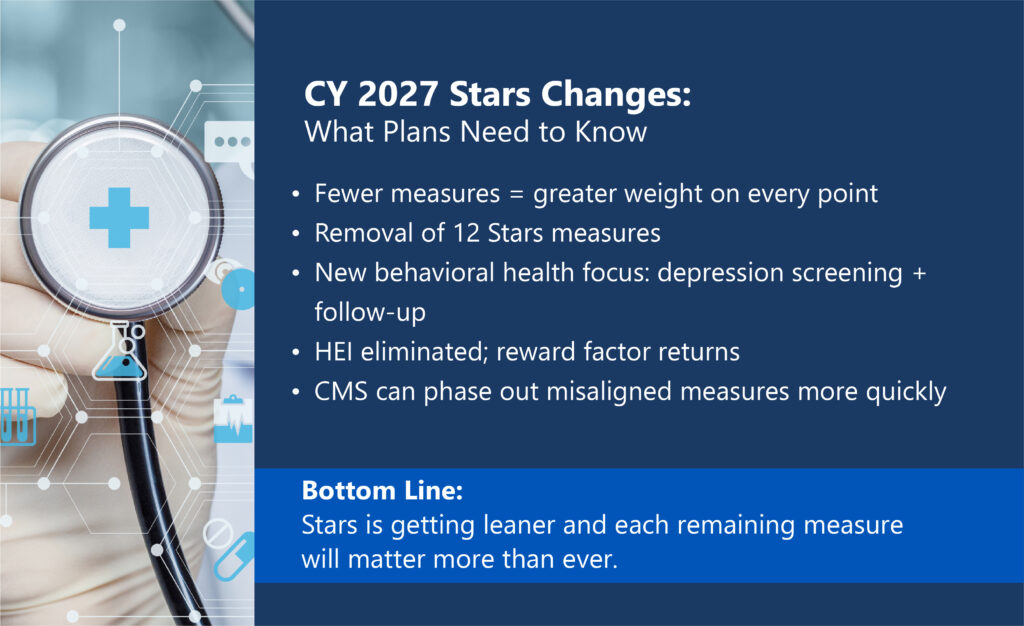
A Leaner, Sharper Stars Program
After much anticipation and industry noise, CMS is finally proposing a shift away from operational obligations and toward measurable member health outcomes, proposing to remove 12 measures, introduce a new depression screening and follow-up measure. This pivot is also in line with the “MAHA” agenda from this administration.
CMs has also proposed not move forward with replacing the Health Equity Index (HEI) with the historical Reward Factor.
Given these changes, CMS simulations suggest 62% of contracts would see no Stars change, around 13% gain a half star, around 25% would lose a half star and one contract losing a full star, with around 9% gaining or losing QBP status.
CMS is explicitly asking for feedback on further simplifying the measure set and methodology while reorienting toward outcomes, prevention and healthy aging.
Targeted Deregulation and Reduced Administrative Burden
CMS proposes to rescind several recent health equity and disparities reporting requirements (UM health equity analysis, QI health disparities activities, public posting) and eliminate the Mid-Year Supplemental Benefits Notice and Multi-Language Insert/Notice of Availability.
Third Party Marketing Organization (TPMO) rules are loosened, with fewer constraints on timing and location of marketing appointments, shorter call recording retention and more flexibility in marketing language, within a “not misleading” standard.
A Deeper Look at Special Needs Plans
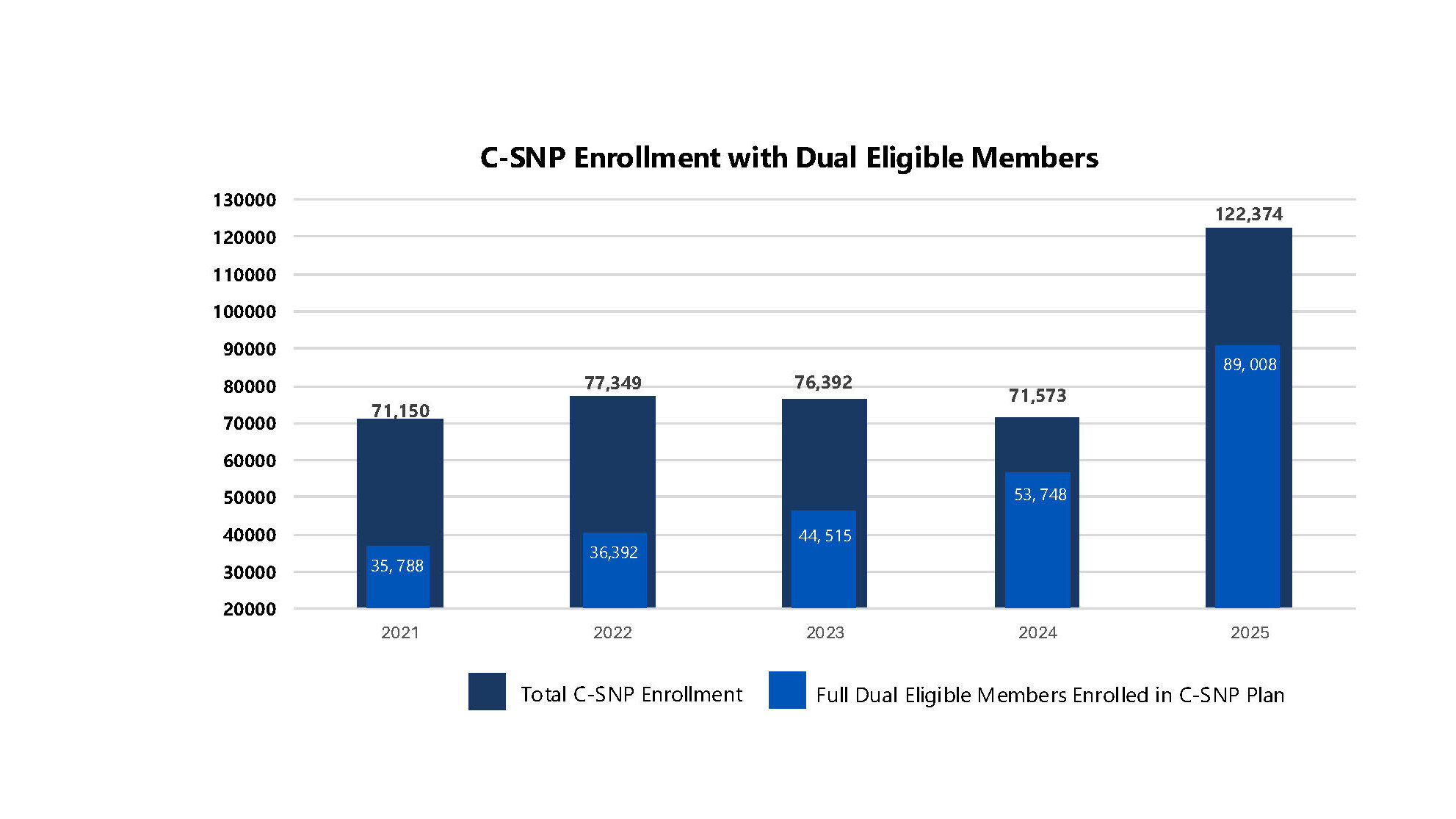
CMS has observed rapid growth in C-SNP and I-SNP enrollment, raising concerns that many of these members may be better served in a D-SNP, where their Medicare and Medicaid benefits can be fully integrated, something C-SNPs and I-SNPs do not provide.
The rule and RFI explore stronger state oversight of C-SNPs/I-SNPs (via SMAC-like requirements), extension of D-SNP “look-alike” policies and enhanced expectations for care coordination and integration.
Future of Risk Adjustment and Stars QBP: CMS Wants Ideas
While no new risk adjustment model is proposed for 2027, CMS devotes significant attention to an RFI on modernizing risk adjustment and Quality Bonus Payments, with an explicit focus on competition, embracing technology and leveling the playing field for smaller and regional plans.
CMS also proposes to broaden access to risk adjustment data for research and oversight, reflecting a growing emphasis on transparency, program integrity and long-term sustainability of MA.
CMS is seeking information on how artificial intelligence can be leveraged alongside current or future risk adjustment methodologies.
The Net Message: CMS is willing to pull back on some administrative and reporting requirements but only if the industry steps up with credible, data-driven proposals to advance quality, integration, transparency and member value. This program isn’t going anywhere but changes are needed to ensure its long-term viability and longevity.
Stars Ratings: A Smaller Set with Bigger Consequences: What CMS is Proposing?
Key changes to the Stars program in the CY 2027 proposed rule include:
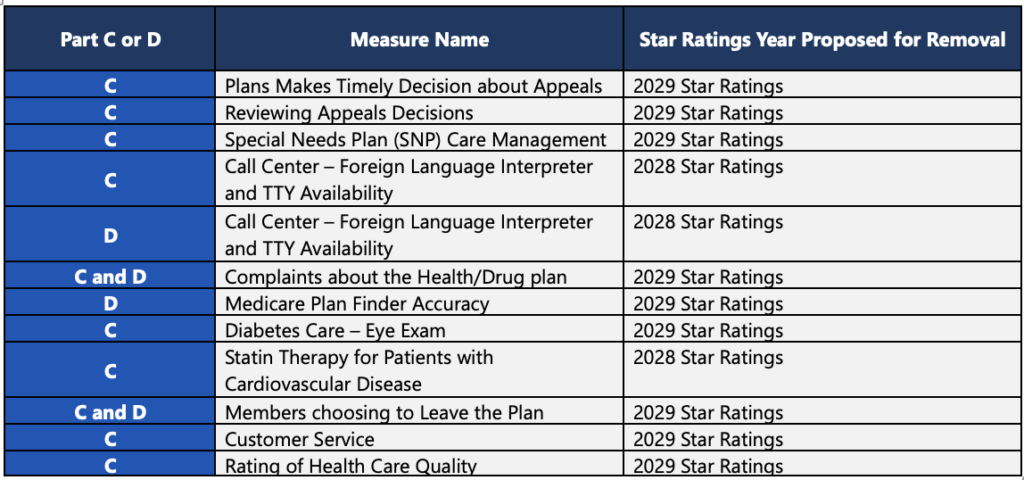
Removal of 12 measures across Part C and D, including:
Administrative and operational measures such as appeals timeliness, appeals review, SNP care management, call center interpreter/TTY availability and plan complaint metrics.
Select clinical or process measures, including diabetes eye exam and statin therapy for patients with CVD.
CAHPS experience measures including customer service and rating of health care quality.
Addition of one clinical measure: Depression Screening and Follow-Up (Part C), reinforcing CMS’s growing focus on behavioral health.
Elimination of the Health Equity Index (HEI) or EHO4All and reinstatement of the historical Reward Factor for contract performance.
Faster, more flexible measure removal, allowing CMS to retire measures through rulemaking when low reliability, misaligned with current clinical guidance, or retired by the steward.
CMS’s impact simulations indicate:
Around 62% of contracts see no change in overall Star Rating
Around 13% gain 0.5 star
Around 25% lose 0.5 star
1 contract loses 1.0 star
Around 9% of contracts gain or lose QBP status
What It Signals
The Stars Program is not being gutted (for now). CMS even acknowledges that the technical expert panel recommended more measures, to dilute a plans ability to only focus on a handful of “critical ones”. In our opinion, CMS could be gearing up for a new plethora of outcomes based and health/behavior health measures soon. Especially in this new “MAHA” world, CMS is reinforcing clinical outcomes, preventive care and member experience as the core levers of Stars. Results based and data driven is the name of the game here. Look to measure stewards for changes to measures and new possibilities.
Implications for Plans
Every plan needs to immediately refresh and re-run Stars models with the proposed changes, including new/removed measure changes and weighting implications. A fulsome examination of vendor partnerships, strategic priorities, technology stack and intervention plan needs complete, to ensure alignment toward CMS’s signaling changes. This includes a rebalance of interventions toward high-impact clinical measures such as chronic condition management and behavioral health. Lastly, decisions are made by those who show up…engage in the RFI process, offering data on outcomes and operational feasibility.
Administrative Simplification and Targeted Deregulation
A second through-line in the proposed rule is deregulation, removing certain requirements that have grown up around MA plans in recent years.
Key Proposals
CMS Proposes To:
Modify the SEP for provider terminations, creating a straightforward SEP for Provider Terminations that begins when enrollees are notified.
Rescind communication and reporting requirements, including:
Mid-Year Supplemental Benefits Notice
Multi-Language Insert or Notice of Availability
UM Committee health equity requirements
Quality Improvement Program health disparities requirement
Loosen TPMO and marketing constraints, including:
Removing the 48-hour waiting period between Scope of Appointment and personal marketing appointment.
Allowing marketing events to immediately follow educational events in the same location.
Permitting SOA forms to be obtained at educational events.
Moving the required disclaimer from “first minute” to “before benefits discussion.
Allowing superlatives as long as statements are accurate.
Shortening recorded call retention to 6 years, or possibly 3, while keeping enrollment record retention at 10 years.
Implications for Plans. Recalibrate, don’t over-relax. Even with looser marketing timing and language rules, strong internal monitoring and oversight remain essential to ensure guardrails are clear and consistently followed. Reinvest freed resources from reduced administrative tasks into more high value areas.
D-SNPs, C-SNPs, I-SNPs, and the Next Phase of Integration
The industry has experienced an explosion of growth in C-SNP and I-SNP enrollment and CMS has noticed. In this rule, CMS provided evidence that many of these members that are dual eligible and may be better served in a D-SNP, where their Medicare and Medicaid benefits can be fully integrated, something C-SNPs and I-SNPs do not provide.
Key Provisions and Ideas
Passive Enrollment for Integrated D-SNPs
Removes the requirement for “substantially similar” networks and instead requires 120 days of continuity of care and adequate care coordinator staffing.
Continuity of Enrollment for Full-Benefit Duals
Allows D-SNPs in HIDE or coordination-only structures to maintain enrollment for full-benefit duals in Medicaid FFS.
RFI on C-SNP/I-SNP Oversight
Possible SMAC requirements for C-SNPs and I-SNPs with high dual enrollment.
Extension of D-SNP look-alike contracting limits.
New care coordination expectations and focus on mental health and substance use disorder management.
Implications for Plans. CMS expects more integration between Medicare and Medicaid, not segmentation. The more closely aligned these programs are, ultimately provides a better experience for the member. Plans should reevaluate duals portfolio strategy and model the financial and operational impact of SMAC or look-alike rules. They should also continue to strengthen state partnerships and care coordination infrastructure and embrace AI/automation technology. Lastly, plan leaders should prepare for a regulatory environment that favors integrated D-SNP over C-SNPs and I-SNPs.
Future of Risk Adjustment and Stars QBP
Although CMS did not meaningfully commit to or propose sweeping change to Risk Adjustment or Quality Bonus Payments, CMS did ask, “what should the next generation of MA payment, risk adjustment and quality policy look like?”. CMS continues to express a willingness and frankly an eagerness to hear from the industry. CMS is seeking to enhance competition and level the field for smaller and regional plans, something that has been needed for some time now. They also are seeking perspectives on how artificial intelligence can be leveraged and how to improve accuracy and integrity of risk adjustment including expanding access to risk adjustment data for research and oversight. Although not reflected in this proposed rule, make no mistake, big changes are coming for Risk Adjustment either in a future proposed rule or through a mandatory Innovation Model.
Implications for Plans. Plans should be responding to CMS’s RFI and provide data-driven comments that balance fairness, accuracy and predictability in the Risk Adjustment program. Any small or regional plan should highlight regional plan challenges and propose practical remedies. Lastly, plans should seek to link innovation and data to measurable member outcomes.
Other Notable Proposals
SNP MOC Submission moves earlier in June with two off-cycle update windows (Jan–Mar, Oct–Dec).
Part D PDE Audit Appeals gains a new three-level process with defined rights and timelines.
Strategic Roadmap for Plans
Leading organizations should act now on three fronts:
Policy and Advocacy: Create a coordinated review strategy for this proposal to ensure thorough, well-supported and meaningful comments are provided back to CMS. Respond to RFIs related to Stars measure set, duals policy, risk adjustment modernization and TPMO rules.
Analytics and Scenario Modeling: Re-forecast Stars and QBP outcomes. Map dual populations across product types and simulate regulatory changes. Quantify administrative burden reductions and plan reinvestment opportunities.
Operating Model and Governance: Refresh Stars and Quality governance to reflect outcome-focused measures. Update marketing and compliance policies for new TPMO rules. Strengthen duals integration, care coordination and continuity processes.
Closing Thought:
The reality is that the 2027 Proposed Rule for Medicare Advantage, is not simply a minor adjustment or a small tweak to a legacy program, it is the opening move in a broader Medicare Advantage reset. The convergence of new technology, a changing regulatory environment and an intensely dynamic marketplace is making it impossible to succeed using yesterday’s playbook. Product strategy, benefit design, network and care models, Stars and quality, risk adjustment, duals integration, sales and marketing, data and technology, all of it is in scope. Old models of success need to be challenged and future models of success need to be invented and operationalized now.
Read the overview here
This is the first Medicare Advantage proposal of the new administration and it is a clear signal that more structural change is coming. Stars changes are here, and more are inevitably on the horizon. Risk adjustment will be changed, the only question is when and how, not if. Through the RFIs in this rule and related Innovation Center work, CMS is explicitly asking the industry to help design the next era of Medicare Advantage. Decisions are made by those who show up and plans that engage thoughtfully, offer data driven perspectives and put forward practical ideas will be better positioned for whatever comes next. ProspHire is here to help you navigate the flurry of change and take a thoughtful, methodical approach to this new reality. We partner with health plans to reassess and modernize Medicare Advantage operating models, from Stars and risk adjustment to product and network strategy, duals and SNP portfolios, data and analytics and sales and marketing governance. We can help you game plan scenarios, quantify impact, redesign processes and craft clear, compelling responses to RFIs and proposed rules. The Medicare Advantage reset is underway. The organizations that thrive will be those willing to throw out outdated assumptions and start designing their next model of success today.
Medicare Advantage (MA) continues to be one of the most competitive and highly regulated sectors in healthcare. With shifting CMS requirements, evolving member expectations and an increased focus on quality outcomes, health plans face growing pressure to balance compliance, cost and performance. ProspHire’s Medicare Advantage Practice helps health plans thrive in this complex environment, bringing hands-on execution experience across Stars performance, risk adjustment, cost savings initiatives, member engagement and operational improvement.
In this Q&A, we sit down with Andrew Bell, Medicare Advantage Practice Leader, to explore the trends shaping MA today, the evolving market and how ProspHire partners with clients to deliver measurable impact.Medicare Stars landscape.
Section 1: Inside the Medicare Advantage Market
What are some of the biggest challenges facing Medicare Advantage health plans today?
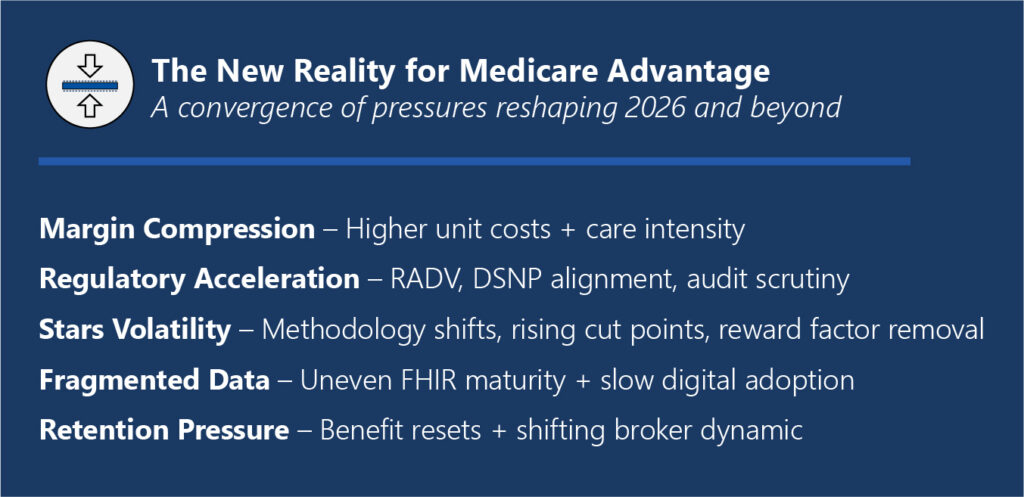
The Medicare Advantage space remains amid massive and fundamental change. Over the past 15 years, the MA industry has experienced nothing but tremendous growth, a favorable regulatory environment, steadily increasing payments and reimbursements and growing membership. As the industry emerges from the unusually favorable conditions of the past few years, plans now face a fundamentally new operating environment. This Medicare Advantage reset is happening at a time when several major pressures are converging.
Margin compression + utilization volatility: Higher unit costs, post-COVID acuity and site-of-care shifts are outpacing bid assumptions.
Regulatory whiplash: Rapid measure changes, audit intensity (RADV), supplemental benefit scrutiny and DSNP alignment rules tighten the screws.
Data fragmentation: Clinical data liquidity is still uneven; FHIR maturity varies by partner; Internal ops aren’t fully digital-first.
Distribution + retention pressure: Benefit resets strain retention; Broker dynamics and member friction affect mix and persistency.
These market pressures, combined with outdated models for success, will be the reason many Medicare Advantage plans will struggle in the near term.
What opportunities exist for plans to differentiate themselves in an increasingly saturated MA market?
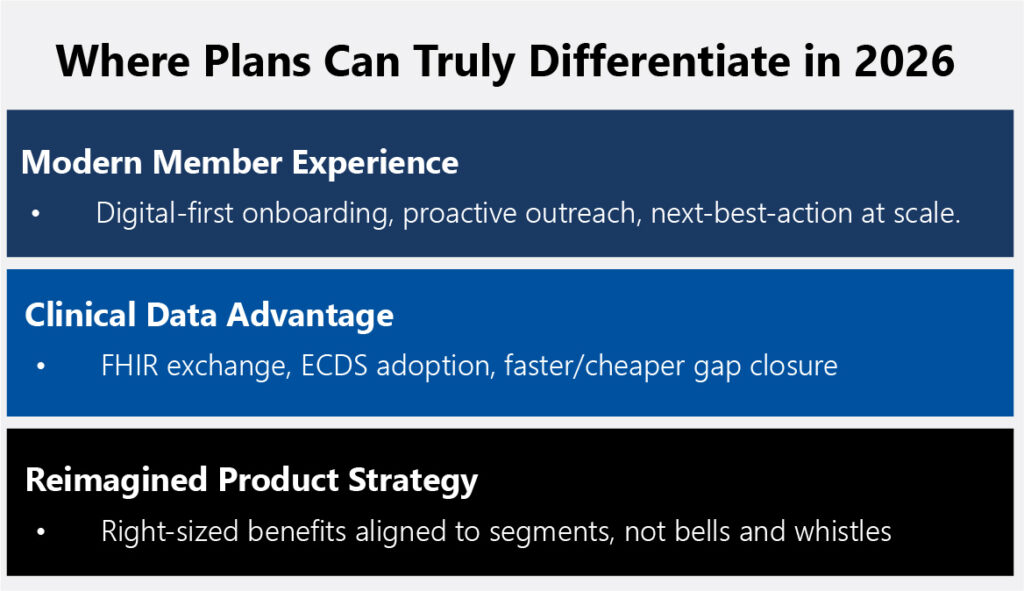
In terms of “real” market differentiation, recent years have shown that Medicare Advantage plans have had little “true” differentiation. Plan benefit packages, supplemental benefits and provider networks were nearly identical across markets and carriers. Now, in the age of the Medicare Advantage reset, plans have the tremendous opportunity to truly differentiate themselves not only to members but to providers and regulators.
Member experience in the modern age: The adage of Medicare Advantage members was that they were primarily baby boomers with little to zero interest in digital engagement and experience. Snail mail, direct to consumer outreach and traditional outreach models worked until they didn’t. In fact, this demographic is more tech savvy than ever, not to mention that in five years the first Gen X’er will be Medicare eligible. This means that plans have the true opportunity to treat member experience and engagement like banking and retail and bring it into the modern age, frictionless onboarding, proactive outreach and next-best-action at scale.
Clinical data advantage: CMS and other regulating agencies continue to push for new and innovative advances in interoperability and digital quality measurement. This top-down approach to innovation can only move as fast as the regulators care to move and the moment is ripe for forward thinking plans to move fast and truly embrace this digital future. Plans should focus on superior ECDS/digital data capture that closes gaps faster (and cheaper) than competitors and FHIR based interoperable data exchanges to further democratize data and place the member at the center.
Reimagined product strategy: Every plan must do more with less. The age of overly rich benefit packages ripe with all the bells and whistles is gone. Plans need to really consider their market, their specific membership needs and right-size benefits and PBPs around segments (e.g., DSNP, chronic cohorts) rather than trying to be everything to everyone. This reimagined product strategy will certainly be “less rich” than previous benefit cycles but will be a better reflection of the current reality and ultimately will be more sensible and practical as a matter of financial prudence.
Section 2: Driving Stars Performance Excellence
Stars Ratings continue to be a major performance driver for Medicare Advantage organizations. What trends are you seeing across the industry?
It’s impossible to separate the larger Medicare Advantage reset from the Stars trends and pressures we’re seeing across the industry. In many ways they are inextricably linked. Stars leaders have less discretionary spending at their disposal to throw at late HEDIS blitz’s or that intriguing new vendor to pilot. Leaders will have to scrutinize every dollar spent and focus on what truly delivers value and ROI.
Another area of interest is how plans are navigating the rapidly changing Stars regulatory and rule environment. The industry has seen more change in the past two years than we’ve experienced in the past many years. New measures, new methodologies and new considerations all crashing at the same time is putting pressure to Stars leadership and health plan leadership to maintain the Stars revenue.
Many plans have in the past resorted to large regional or national contracts to concentrate Stars performance on one mega contract. This strategy has yielded great success to those national players by insulating Stars risk and maximizing Stars related revenue. However, the recent Stars regulatory changes are flipping that old model on its head, and many national players are scrambling to understand their exposure (see the most recent Humana Stars loss and the impact to their revenue). I think that this is a big wake up call to health plan leaders who may have taken their prior Stars success for granted. Many plans (even those with consistent 4.0+ success) are taking the time to evaluate their programs and determine whether a new path needs charted, one with less Stars exposure and tighter controls in place.
Last but certainly not least, what remains is the uncertainty on the future of Stars itself. The long-standing program is facing growing criticism from Washington DC policy circles, including groups like the Paragon Institute, as well as from MedPAC, which has repeatedly called for changes to the program and the elimination of quality bonus payments. Wherever the program ends up in the near term, one thing is for sure, changes are coming and plans will be forced to react.
How can plans improve or sustain their Stars Ratings amid regulatory tightening and the new Stars reality?
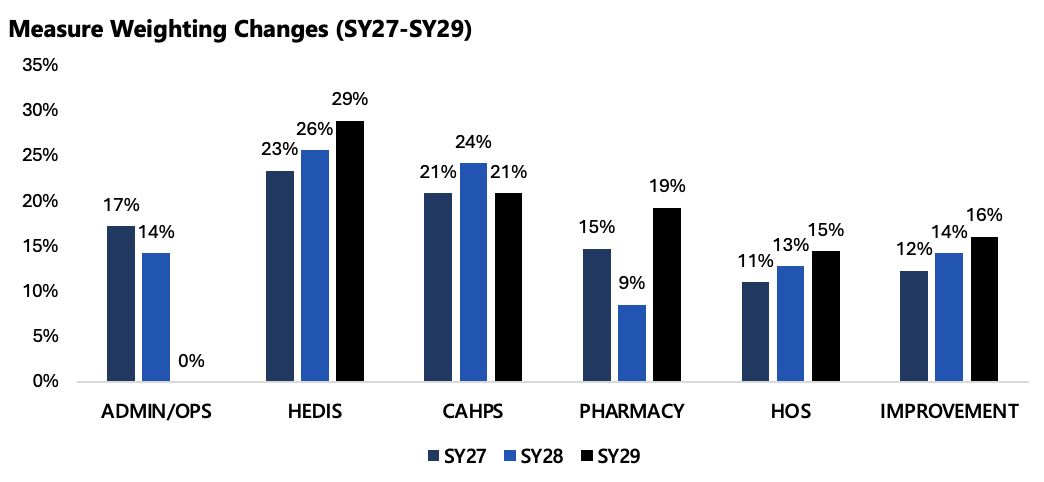
Plans looking to maintain or grow their Stars Ratings in a period of regulatory tightening and volatile cut points need a dual approach. In the near term, leaders should concentrate on interventions across the sub-set of measures still within reach for the current cycle, focusing on the controllable levers that can meaningfully shift outcomes before submission. Simultaneously, they must begin rebuilding the operating model for the next three years, anticipating the structural realities of future Star Years (SY27–SY29), including digital measure adoption, reward factor removal, the EHO4 all measurement, integration of AI and automation into workflows and finally reduced resources available.
A major driver of Stars success is mastering both the denominator and numerator. Plans must “own the denominator” through eligibility hygiene, attribution accuracy and encounter completeness to minimize avoidable misses and ensure members are correctly represented. Time and time again we see that plans struggle with data capture on the front end, leading to data leakage and numerator devaluing. On the numerator side, success increasingly depends on a reimagination of the vendor stack, standardizing clinical data ingestion, prioritizing FHIR-first architecture, automating evidence capture and compressing cycle times from weeks to days. This operational rigor allows teams to act on near-real-time information rather than retrospective data.
Member experience remains a differentiator. CAHPS performance cannot be treated as a once-a-year campaign. It must be embedded as an operating philosophy that influences every member touchpoint, access, communication and trust. Finally, executive visibility is critical. Weekly Stars reporting at the contract (and potentially PBP) level and the measure level, with a clear path-to-goal and owner accountability, ensures leadership alignment, proactive intervention and real-time decision-making as performance shifts throughout the year.
What practical steps can organizations take to enhance performance and avoid the rush of year end?
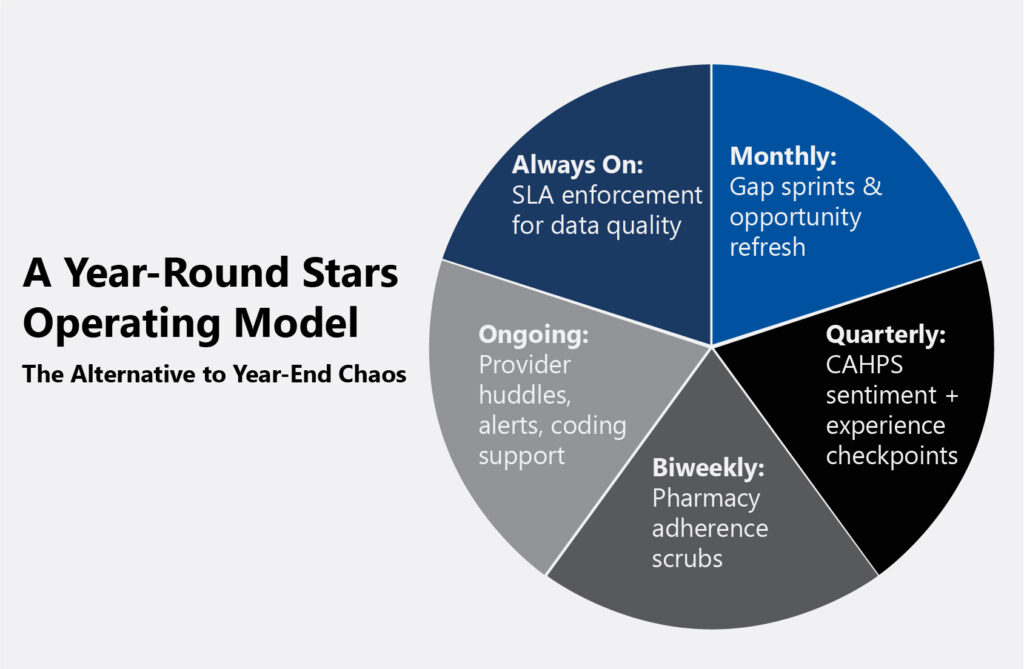
Sustained performance comes from embedding Stars management into year-round operations rather than relying on end-of-year surge efforts. A 12-month playbook lays the foundation and helps to maintain momentum: monthly gap sprints to close measurable care opportunities, quarterly CAHPS reviews to monitor member sentiment, biweekly pharmacy adherence scrubs to improve medication persistence and ongoing provider performance huddles to reinforce expectations are a few of the many ongoing efforts that need to be deployed.
In addition, provider engagement should be a crucial component of the 12-month playbook. This goes beyond the table stakes of providing visit “starter kits”, coding education, alert systems embedded into care delivery system and performance incentives. With the growing adoption of near-real-time reporting for quality measures through FHIR-CQL adoption, plans and providers can begin to close the gap that exists between them, and start to have more meaningful, real-time discussions of member care.
Data accountability is equally important. Service-level agreements (SLAs) for both internal teams and vendors must define timeliness, completeness, and reconciliation standards to ensure data reliability. Enforcing these SLAs helps minimize lag, rework and reporting discrepancies, allowing quality and Stars teams to make decisions based on accurate, current information rather than chasing data fixes in Q4.
Section 3: Data, Analytics and Member Engagement
How can data and analytics be better leveraged to drive Stars, Risk Adjustment and Quality Performance?
Accurate, complete and streamlined data sets serve as the cornerstone of high-performing Stars, risk adjustment and quality outcomes. This level of data integrity enables plans to pinpoint opportunities, respond quickly to performance gaps and drive meaningful operational improvements. Plans can no longer rely on the status quo, evolving regulatory expectations and digital quality requirements demand a proactive transformation of data strategy and infrastructure. The most effective organizations are reengineering their data foundations to unify clinical and administrative sources into a single analytics pipeline.
A modern approach leverages FHIR-based ingestion, standardized mapping, CQL-driven measure calculation and near-real-time dashboards to transform raw data into actionable intelligence for Stars, risk adjustment and quality programs. By incorporating opportunity scoring, plans can prioritize high-value data source, such as HIEs, EHRs, labs and retail clinics, based on timeliness, yield and cost-per-closed-gap, while closed-loop analytics drive continuous improvement by triggering next-best actions and measuring hit rates, not just identified gaps.
Where do you see the greatest opportunity for innovation in MA, whether through technology, partnerships or process improvement?
The next wave of innovation in Medicare Advantage will be defined by digital quality measurement, interoperability and artificial intelligence, all buoyed against the changing tides of regulatory or agency action. Transitioning from hybrid to fully digital measurement unlocks faster, lower-cost numerator capture and real-time performance visibility, all supported by the growing need for interoperability that enables seamless clinical and administrative data exchange across Medicare. Paired with this, artificial intelligence will also continue to play an emerging role, not as a replacement for human decision-making but as a prioritization engine that predicts which members are most likely to close gaps, which interventions will be most effective and at what cost.
Section 4: Partnering with ProspHire
How does ProspHire’s Medicare Advantage Practice uniquely support health plans navigating these challenges?
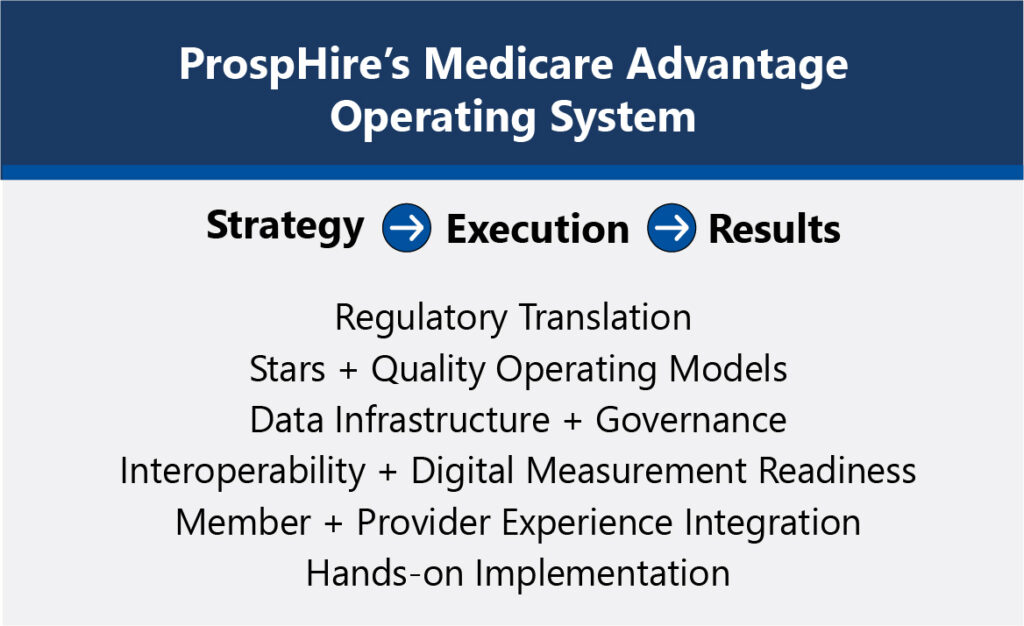
ProspHire’s Medicare Advantage Practice combines deep regulatory expertise with hands-on implementation capability, enabling plans to translate strategy into sustained performance. Our team bridges the gap between CMS rules and operational reality, turning regulatory language into actionable playbooks, KPIs and accountable workflows. We support clients in building comprehensive Medicare Advantage operating systems that deliver transparency into compliance, benefit administration, care management, member experience and overall operational effectiveness. Our operating systems are complete with clear ownership, measure actions and executive-level dashboards that track progress toward organizational goals.
ProspHire partners with plans to take a forward-looking, proactive stance on regulatory and operational readiness. Unlike traditional advisory firms, we embed alongside client teams to build and stabilize these capabilities, not just design them. ProspHire’s delivery model ensures plans have the data infrastructure, governance and workflows needed to sustain performance year over year.
Looking ahead, what should health plans be prioritizing as they navigate the Medicare Advantage reset?
As the Medicare Advantage market grows increasingly complex, the key to long-term success lies in aligning compliance, quality, total cost of care and operational effectiveness under one strategy. ProspHire brings deep executional expertise, translating strategy into action and driving results that elevate Stars Ratings, member satisfaction and financial outcomes. With a view across data, delivery and engagement, ProspHire helps health plans not only meet CMS standards but set new benchmarks for excellence in Medicare Advantage.
The Medicaid market continues to evolve amid shifting regulatory priorities, state-level variations and economic pressures. As health plans, providers and agencies adapt to changes in funding, eligibility and oversight, the need for flexible strategies and expert execution has never been greater. In this updated Q&A, ProspHire’s Medicaid Practice Leader, Julie Evans, discusses the challenges, innovations and forward-looking strategies shaping Medicaid in 2026 and how ProspHire partners with clients to drive meaningful, measurable impact.
Section 1: Current Landscape & Pressing Challenges
What are some of the most pressing challenges that healthcare organizations face in navigating the Medicaid landscape, particularly considering recent regulatory changes?
Recent regulatory changes are most impactful with consideration to Medicaid eligibility, accessibility and sustainability. Looking ahead, as redeterminations become more frequent, work requirements become a reality and marketplace costs increase, the currently or formerly eligible Medicaid population face uncertainty. For healthcare organizations, this translates to coverage gaps, member abrasion and high administrative costs. Payors will seek to support their membership in understanding their eligibility and support in the administrative requirements to maintain coverage, but for those who temporarily lose coverage or go for an extended period without coverage, additional complications arise. The acuity of Medicaid members has increased, particularly as an outcome of the ending of the COVID-19 public health emergency redeterminations. As individuals lose or go without healthcare coverage, preventive care and health issues go unaddressed. Over time, we can expect that this will impact acuity and cost of care further, as preventive care is bypassed and members are faced with more complex health needs.
As financial pressures and administrative complexities continue to grow, how do we keep the member and care delivery at the forefront of Medicaid?
Financial and administrative burdens aren’t going anywhere as Medicaid will continue to face these challenges by nature of the program. Likewise, the pressure to drive improved health outcomes will also continue to exist and to achieve the desired health outcomes with a health plan’s wallet and administrative requirements in mind, there are several opportunities.
Improved member engagement in preventive care and care management programs result in improved cost of care; therefore, driving a human-centered strategy will result in improved financial performance.
Leveraging administrative data requirements to tell the human story will create added value in regulatory and quality operations.
Removing administrative burdens on member-facing roles wherever possible through technology and operational efficiencies will allow the member and human connection to be the focus.
Build trust and partnerships with the community and the community-based partners to engage with and improve care delivery. When members are being met where they are and their ample needs outside of medical care are being met, we will see improved engagement, outcomes and satisfaction.
As a reminder, Medicaid looks different not only across states but the needs of Medicaid members can vary down to the zip code level. The strategies are theoretically similar across health plans but execution should be deliberate with consideration to regional membership. Take care of the members to see improved outcomes and improved financial performance, allowing for reinvestment into operational efficiencies, staffing and technology to drive innovation and alleviate the “burden” of administrative and regulatory activities.
Section 2: ProspHire’s Approach & Methodology
How does ProspHire help clients drive innovation and sustainable improvement in Medicaid?
One of ProspHire’s core values is relationships. As we seek to drive innovation and sustainable improvement in Medicaid, our first step is to understand each health plan’s unique population and regional priorities through relationships with Medicaid beneficiaries, customer facing teams and community-based providers.
State regulations and region-specific needs are the foundation of Medicaid services and pose unique guardrails for our clients. While state regulations are rigid and defined, region-specific needs vary and evolve leaving room for innovation. Through a customer-centered approach, we seek to understand, rather than assume, and drive innovations that are inspired by the customer, leading to desirable and sustainable improvement.
ProspHire partners with our clients to amplify the voice of the customer through the ideation and execution of their innovations by means of strategic initiatives in alignment with organizational priorities.
How does ProspHire stay on top of the evolving Medicaid regulations and policies and how do you ensure your clients remain compliant?
Read, watch, listen and react. Like many of our clients, we stay up to date on industry changes, trends and discussions to prepare ourselves and others to react to our evolving environment. This includes the ever-changing regulatory requirements and discussions at the federal and state level. Our attention to detail and quality assurance practices help us work in partnership with our clients and their legal and compliance teams to drive results and remain agile and in the case of political shifts, prepare for flexibility and adaptability in response to any sweeping or frequent policy changes.
Technology plays a crucial role in modernizing healthcare delivery. How does ProspHire integrate technology solutions into its Medicaid services to improve efficiency and outcomes?
Technology is continuously increasing in significance across healthcare delivery. Most recently our team supported the integration of a new clinical platform to enhance care management, utilization management and reporting capabilities. From requirements gathering to go-live and post go-live risk management and resolutions, our team has been in the weeds, working alongside the client to deliver a multi-state clinical solution. This tool improves efficiency of workflows, decision making and ultimately the delivery of care to the Medicaid population and those who are most vulnerable to adverse health outcomes.
Artificial Intelligence (AI) is another technological advancement that is buzzing as vendors and healthcare organizations find opportunities to integrate AI in the industry. ProspHire focuses on the business and end user when considering AI implementation, supporting health plans through business case development, user stories, vendor or system implementation and readiness and adoption activities. By preparing our clients to utilize the technology effectively, there is a greater return on investment through improved efficiency and outcomes.
Lastly, as quality improvement measurement transitions to digital quality measures (dQMs), health plans will face unique challenges in technology including application programming interfaces (APIs), coding, vendor integration and more in preparation for regulatory requirements driving this shift. The roadmap exists to embark on this transition but many health plans will require project management and subject matter expertise to drive the tactics and execution of this shift to achieve coordination across the organization, assess dQM readiness, conduct successful parallel reporting and ultimately migrate to the dQM model in a timely manner.
Plans have different technological needs depending on the current state of their operations and we partner with our clients to integrate the solutions that are prioritized in alignment with organizational goals to deliver improved member and operational outcomes.
Section 4: Data-Driven Insights and Equity
Can you talk about the importance of data analytics in Medicaid projects and how you use data-driven insights to inform decision-making and strategy development?
Social Determinants of Health (SDOH) and health equity efforts have led to a shift in the way specific care needs are identified and delivered. A challenge posed by SDOH, and ultimately health equity, is the variation in need based on environmental factors. Through partnerships with community-based organizations and our clients, mutual goals can be achieved by addressing social needs and downstream health outcomes.
To do so, data analytics is crucial. Who is our population of focus? Where do they live? What impact will our intervention have? These are all questions that data can provide insight to. Knowing this, ProspHire has supported population health assessments and data dashboards focused on marrying publicly available data and internal clinical data to support data-driven decision making. These tools support strategic development and inform the who, what and where of many Medicaid projects, specifically those focused on quality.
Section 5: Value-Based Care and Future Outlook
With the rise of Value-Based Care, how do you assist clients in transitioning from fee-for-service to value-based models within Medicaid?
Pay for performance models, shared savings programs, patient centered medical homes, Medicaid ACOs… the many value-based care models, continue to evolve and demonstrate their effectiveness. Our focus is to support the readiness and feasibility of transition followed by the monitoring and controlling of care model commitments. The continuous need to reduce costs and deliver improved quality of care poses a challenge to both providers and payors and leads to the continuous need to reevaluate and refine our reimbursement structures.
Looking ahead, what trends do you anticipate shaping the future of Medicaid consulting and how is ProspHire positioned to address these trends proactively?
As a boutique consultancy with an exclusive focus on healthcare and an emphasis on government programs, ProspHire is well positioned to be adaptive and quickly support our clients in understanding, implementing and monitoring the changes and impacts of regulatory and industry shifts.
One priority in Medicaid that will remain unchanged is the desire to reduce costs and improve quality, an effort that will continue to foundationally drive ProspHire efforts and priorities. As we evaluate the regulatory environment, industry trends and strategies, our goal remains the same – to drive positive change for our clients and the Medicaid population.
The Challenge: Navigating a Shifting Stars Landscape
Medicare Advantage plans are entering one of the most complex and high-stakes Stars cycles to date. As cut points tighten, new measures are added and a greater emphasis is placed on outcomes-based measures, plans are faced with the reality that every decision from governance design to resource allocation carries a lasting impact. Plans can no longer rely on reactive strategies or one-off improvement efforts. Sustained performance now requires foresight, alignment and deliberate planning across all levels of the organization.
What Successful Plans Are Doing Differently
Leading Medicare Advantage plans are shifting from short-term fixes to enterprise-wide Stars strategies that aligns product strategy, technology investment strategy and operational efficiency around sustained performance. These organizations focus on building accountability and clarity through governance structures, use predictive analytics to inform decision making and integrate real-time data to drive decision making at all levels.
As plans prepare for the 2026 measurement year, several priorities stand out:
Governance Optimization: Governance is basic but it is everything. Plans need to do more with less and that means they should be re-evaluating their current models. They need to seek transparent, accountable and cross-functional governance models that drive alignment and ownership across teams.
Align Product Strategy and Stars Strategy: This AEP has been one of the most hectic AEPs in MA history, with more plans exiting the market and reducing service areas than ever before. The gradual shift away from PPOs and toward HMOs is also telling. Plans need to take the opportunity to align current and future product strategies to Stars strategies to prepare for what’s coming in MA.
Stars Analytics and Forecasting: Analytics and forecasting capabilities are table stakes at this point in the Stars game. Plans need to apply those data-driven forecasts and existing competitive intelligence to stay ahead of regulatory changes and cut point shifts. Integrating Stars intelligence capabilities into network contracting, member engagement activities and business planning are a few of the many use cases of this type of data.
Performance Planning and Domain Expertise: Each domain from within Stars carries its own unique set of rules, nuances and minutia. Plans need expertise at the domain level to be able to connect what the data is telling them with the reality of operations on the ground.
Successful plans understand that Stars success is not just about closing gaps; it is about translating insights into coordinated action that drives measurable results year after year.
Our Perspective
At ProspHire, we have led Stars programs from the inside. Our advisory approach helps health plans move from reactive to deliberate, aligning leadership and operations around a shared vision for long-term success.
Think Ahead. Plan Differently.
The path to future Stars success begins with informed, strategic action today. Let’s plan differently for 2026, combining insight with execution and experience with results.
On November 4th, CMS released the Notice of Intent to Apply (NOIA) applications calendar year 2027 for Medicare Advantage Prescription Drug (MAPD) plans. While often viewed as an administrative first step, the NOIA represents a plan’s formal commitment to participate in the upcoming contract year. More importantly, before the NOIA is even submitted, plans must use this moment to articulate their strategic intent by identifying which products to sustain, where to innovate and what new opportunities to pursue in the year ahead.
This is especially critical amid the Medicare Advantage Reset we are experiencing today. Medicare Advantage headwinds are broad and big, such as shifting regulatory targets, potential policy changes under a new administration, heightened audit scrutiny, increased political pressure and increased need to improve and maintain strong Stars and quality performance.
For plans, the CY2027 NOIA cannot be viewed as business as usual. It needs to be treated as a strategic checkpoint. It’s the moment to define your plan’s Medicare Advantage roadmap, reaffirm market goals and set the tone for the entire bid season.
Some key focus areas for this year’s NOIA cycle include:
Product Realignment: The NOIA enables plans to reassess offerings, retire underperforming products and refine benefits to stay competitive while balancing market appeal with cost containment for long-term sustainability.
Special Needs Plan (SNP) Penetration: SNP plans continue to see steady growth, as reflected in the October CMS landscape files. MAPDs that excel in care coordination and member outcomes are well positioned to capitalize on this trend and benefit from the higher rebate margins these plan types offer.
Market Expansion or Retraction: The NOIA period allows plans to evaluate where to grow their footprint and where to scale back, ensuring data-driven decisions on market participation ahead of bid development.
Organizational Readiness: Before committing to a strategic roadmap, plans should carefully evaluate their existing infrastructure and capabilities to ensure they can operationally support future goals. A sound strategy requires not only vision, but the processes, systems and resources to bring it to life.
As the MAPD landscape continues to evolve, the CY2027 NOIA marks more than the start of another bid cycle. MAPD plans that make the time now to realign, innovate and set a clear goal for 2027 will be well positioned when bids are submitted.
At ProspHire, we have been partnering with health plans for over a decade, navigating this critical period with clarity and confidence by helping organizations strategically plan for sustainable growth, operational readiness and long-term success in the evolving Medicare Advantage landscape. If you are prepared to chart a new path forward, embracing the Medicare Advantage Reset and exploring new models for success, not anchored to the past but positioned for the future, let’s have a conversation.