Typically, any form of audit is considered an organizational risk where time, resources and materials are invested to mitigate penalties. Ideally, this means $0 owed in the final audit findings. The HHS-RADV audit is an exception, where 96 of 295 individual, non-catastrophic HIOS contract holders received a total of $93.4M in transfer adjustments in 2021 because of the audit findings.[1]CMS is willing to reimburse organizations for HCCs found during the audit that were originally not submitted or incorrectly coded during the benefit year submission process. For this fact, ProspHire perceives the HHS-RADV audit as an opportunity instead of a liability and encourages organizations maturing in their ACA risk adjustment operations to share this view.
Establishing a proactive and well managed HHS-RADV audit process is a recommended early step in the journey to best-in-class Risk Adjustment operations. Risk Adjustment benefit years are never operated in isolation and there is always a new benefit year with encounter submission, prospective and retrospective programs which require diligent attention. A common trap when managing these competing priorities is to rely on the contracted Initial Validation Audit (IVA) Service Vendor to manage the HHS-RADV audit with minimal oversight. Unfortunately, the best IVA vendor in the market will likely deliver a substandard outcome unless they are actively managed and supported by the health plan throughout the audit.
ProspHire encourages Risk Adjustment teams to proactively manage 3 crucial areas of the HHS-RADV audit process.
Chase List Construction – Identify and prioritize appropriate charts for the IVA vendor to retrieve.
Chart Retrieval – Review the IVA vendor progress to identify priority charts and leverage provider relationships to acquire the charts the IVA vendor could not.
Chart Coding – Review and challenge IVA vendor coding interpretations as appropriate and identify additional diagnosis codes that were not submitted on an encounter.
Dedicating the resources to establish a best-in-class HHS-RADV operating model early in the tenure of the ACA contract can realize value in the short-term by reducing the financial impact of operational shortfalls throughout the benefit year. This will reduce future financial headwinds and increase the chance for a tailwind while other Risk Adjustment programs are being optimized. Effective HHS-RADV audit operation benefits are not limited to short-term value. A maximally effective HHS-RADV audit operating model will mature with the Risk Adjustment department over time, transitioning from a final HCC recapture opportunity to an effective risk mitigation safeguard. As the HHS-RADV audit for 2023 Benefit Year is commencing, organizations with a history of negative adjustments to Risk Adjustment state transfer results need to accelerate the formation of their best-in-class HHS-RADV audit operating model for immediate value realization while minimizing disruptions to Risk Adjustment program operations for 2024 Benefit Year.
ProspHire can help by being the catalyst to accelerate the operating model development. We offer subject matter experts, project managers and staffing resources to guide and coordinate the Risk Adjustment team in conjunction with the IVA vendor. Most organizations require support to define and manage operations for the first year to enable leaders and staff to gain the experience to be independently successful. Typical deliverables are job aides, governance models, playbooks, process maps, resource estimates and tools for teams to continue to operate a best-in-class HHS-RADV process for years to come. Contact us today while there is still time to make this year the best HHS-RADV audit outcome in the history of your health plan.
Conduct Lessons Learned from Medical Record Review Season Activities
At this point in the year, we are also approaching the mid-way point for SY2026 and this year becomes more critical as member experience weighting shifts from a 4x to a 2x. Plans must ensure that they are organized, have their strategy in place and keep a pulse check on major changes from the last Star Year.
What should you be doing right now
There’s no time like the present: Every day is critical in Stars. Whether it is integrating and aligning data sources, planning and implementing new interventions or developing robust strategies to address gaps from the prior year – start acting today.
Buy-in and commitment are enhanced: Ensure that you have complete buy-in from leadership and commitment to put Stars as a priority. Stars cannot be done off the side of the desk; you must continuously refine your strategy to meet the organization’s goals.
Spotlight on training and education: The Stars program is constantly undergoing changes. It’s important to allocate time to educate your organization on the broad implications Stars has across all areas of business.
Having a year-round CAHPS strategy to consistently focus on member experience and engagement is essential. It’s critical to utilize the feedback from the SY2025 CAHPS survey to inform additional strategies and improved messaging to members.
At ProspHire, we continue to partner with health plans, to offer insights, analyze and execute strategies to improve Star ratings. Do you need support developing the right SY2026 execution strategy? Let’s have a conversation.
We are thrilled to sit down with Lauren Miladinovich, CEO, Managing Principal and Co-Founder of ProspHire. With a profound commitment to enhancing healthcare delivery and execution, Lauren has taken ProspHire to new heights, offering invaluable expertise and innovative solutions to clients across the healthcare landscape.
As CEO and Managing Principal, what overarching principles guide your leadership approach?
My leadership approach is grounded in several core principles: transparency, excellence, integrity and fostering a people-centric culture. Central to this approach is prioritizing open communication through clear, concise messaging and active listening. I encourage teamwork and empower individuals to take ownership of their work to enhance engagement and innovation within our team. Upholding high standards of excellence is a constant pursuit, as we are committed to continual improvement and embrace a culture of learning. Integrity is non-negotiable, as we hold ourselves to the highest ethical standards to build trust and credibility. Additionally, we prioritize the well-being, professional development and diversity of our team members, recognizing that investing in our employees is essential for our collective success. By consistently reinforcing our mission and values and integrating them into our daily operations, we ensure alignment and drive collective success for ProspHire and our clients.
What do you see as the most pressing challenges that healthcare organizations face in terms of delivery and execution? How does ProspHire address these challenges?
The most pressing challenges often revolve around operational efficiency, regulatory compliance and adapting to evolving healthcare landscapes. To address these issues, we leverage our deep industry expertise to help clients develop effective strategies or to execute the strategies that they already have. Our talented team of healthcare consultants bring the knowledge and experience needed to work closely with clients, fully understanding their business and becoming an extension of their team.
Collaboration is crucial in consulting engagements. How does ProspHire build collaboration both internally among team members and externally with clients to achieve successful outcomes?
Collaboration is indeed crucial in consulting engagements. At ProspHire, we prioritize building strong collaboration both internally among team members and externally with clients. Internally, we build a culture of collaboration through cross functional teams, regular knowledge sharing sessions and open communication channels. We ensure that all team members understand the goals, objectives and desired outcomes to help everyone stay aligned and work towards a common purpose. It’s important to create an environment built on trust and respect for team members to feel confident in sharing their thoughts and ideas.
Externally, we believe in building strong relationships with our clients based on trust, transparency and effective communication. We engage in collaborative workshops, co-creation sessions and regular progress updates to ensure alignment and understanding of goals and expectations. By working closely with our clients as strategic partners, we can leverage their insights and domain knowledge to develop solutions that address their unique challenges and drive successful outcomes.
Additionally, we celebrate success. We celebrate small wins and large milestones together to acknowledge achievements and recognize each other.
As a leader in the industry, what trends do you foresee shaping the future of healthcare consulting? How is ProspHire positioning itself to stay at the front of these developments?
There are several pivotal trends shaping the future of healthcare: digital transformation, data analytics, value-based care, regulatory compliance, population health management and interoperability. To maintain our edge, we invest in talent development, building strategic partnerships, customizing solutions, engaging in thought leadership and remaining adaptable to changing market dynamics. By staying ahead of emerging trends, leveraging expertise and providing tailored consulting services we aim to continue to deliver value to our clients and solidify our position as an industry leader in the evolving healthcare industry.
As a successful woman leader and founder, how do you champion and support other women in business, both within ProspHire and across the industry?
I have always been passionate about supporting women leaders and building diversity and inclusion in business. I believe that diverse perspectives lead to better outcomes and stronger teams. Within ProspHire, we actively mentor and provide growth opportunities for women, ensuring they have the resources and support to thrive in their careers. We launched a woman in leadership course called ‘In Her Shoes’ in memory of one of our Managing Directors. We have ProspHire Women’s Network which includes in person and virtual events that are educational or an opportunity to network. We also encourage the women in the firm to seek outside mentorship for well-rounded perspectives.
Additionally, we advocate for women in business through partnerships, sponsorships and initiatives that promote gender equality and leadership development. It’s not just about achieving success individually; it’s about lifting others as we climb and creating a more equitable and inclusive future for all.
Reflecting on your journey at ProspHire, are there pivotal moments or lessons that have significantly influenced your approach to leadership and business management?
There have been many moments and lessons learned that have influenced my approach to leadership and business management. Leadership is a skill that requires continuous development and it’s not a one size fits all approach. I’ve worked with many people who had different styles over the course of my career. I’ve found success when I tailor my style to adapt to others. Also, I’ve learned the importance of leading with empathy.
In the early days of ProspHire, our leadership team met weekly, in person and could fit around an 8-person conference table. That was a vastly different experience than it is today with nearly 30 people on the leadership team, mostly virtual and in different geographies. There have been many challenges and changes with the growth of the team and the evolution of a hybrid work environment. Being resilient and open to change has allowed for smooth transitions.
Keeping our mission and values at the forefront of every business decision has been paramount in our success.
What excites you most about the future of ProspHire and the broader healthcare consulting landscape? What do you envision as the next phase of growth and impact for the Firm?
What excites me the most about the future of ProspHire is being able to continue our mission to help our clients provide better access to quality healthcare. Understanding their needs, exceeding their expectations and earning their loyalty is my core focus. We’re making a meaningful impact in healthcare and that drives all of us to want to continue growing.
Giving back to the communities we live and work in is deeply fulfilling. We have a long-standing partnership with Boys and Girls Clubs. We even spend our Prosper Together Day of service with the kids.
We’re always exploring new markets, both geographically and demographically. The potential for reaching new clients and leaders and expanding our footprint opens avenues for substantial growth. Deepening our industry partnerships can amplify our strengths and drive innovation to deliver exceptional value to our clients. The rapid pace of technological innovation presents endless opportunities for us to improve existing processes and streamline operations. Embracing emerging technologies can position us at the forefront of our industry. The future of our Firm holds immense potential for innovation, growth and positive impact. By focusing on these aspects, I am confident that we can build a prosperous and sustainable future for our employees and clients.
Welcome to our Q&A session with Chris Miladinovich, the Co-Founder, Principal and Chief Strategy Officer of ProspHire. With extensive experience in strategy development, business operations and healthcare consulting, Chris has been instrumental in driving ProspHire’s growth and success. ProspHire is renowned for its innovative solutions in healthcare consulting, providing invaluable support to organizations navigating the complexities of the healthcare industry. We have the privilege of diving into Chris’s insights, experiences and perspectives on the challenges and opportunities within healthcare consulting and beyond.
Can you share the inspiration behind founding ProspHire and the journey that led you to where you are today?
Lauren and I founded ProspHire out of a shared vision and belief that there was a better way to build a consulting firm. We both had extensive experience working for other firms, where we witnessed firsthand the challenges of maintaining a strong culture while prioritizing the bottom line.
Driven by a desire to build something different, something more impactful, we set out to create a consultancy where culture wasn’t just a buzzword but the beating heart of everything we did. We wanted to foster an environment where our team could thrive, knowing that happy consultants deliver the best results for our clients.
Our frustration with the status quo fueled our determination to do things differently. We wanted to build a Firm where we could prioritize both the well-being of our team and the quality of our services. And thus, ProspHire was born, with a mission to deliver best-in-class services fueled by a culture of excellence, collaboration and care.
After about two years in business, we took a critical look at our trajectory and realized that to truly excel, we needed to focus our expertise and do something very well. Leveraging our deep experience in healthcare and robust networks within the industry, we made the strategic decision to specialize in serving the healthcare sector. This laser focus allowed us to hone our expertise, deepen client relationships and deliver even greater value to our partners in the healthcare industry.
What are some of the unique challenges you’ve encountered in the healthcare consulting industry and how does ProspHire address these challenges?
At ProspHire, we’re no strangers to the unique challenges that permeate the healthcare consulting industry. Every day we’re fortunate to work alongside our clients, tackling their typical challenges head-on. However, what sets us apart is our recognition that there’s no ‘one size fits all’ solution, even for the most common issues.
Our approach at ProspHire is highly customized to each client’s specific situation. We’ve structured our Firm around this principle, ensuring that every engagement begins with a deep dive into understanding the heart of the problem. Our team is trained to be attentive listeners, adept at unraveling complex challenges and skilled at crafting tailored solutions.
While we encounter similar hurdles across clients, the most unique challenges often arise from external factors like the COVID-19 pandemic, rapid regulatory changes and the diverse economic needs of individual clients. Despite these variables, our approach remains steadfast. We listen intently, seek to understand and leverage our collective experience – which includes the successful delivery of billions of dollars in value across our national client portfolio – to drive impactful solutions.
Whether it’s navigating the complexities of a post-pandemic healthcare landscape or adapting to swiftly changing regulations, ProspHire stands ready to partner with our clients, providing not just consultancy but a commitment to implementing and standing behind the solutions we deliver.
As the Chief Strategy Officer, what key strategies has ProspHire implemented to stay ahead in the rapidly evolving healthcare landscape?
My primary responsibility is to ensure that we not only set ambitious goals but also effectively communicate and achieve them. While we have our typical corporate objectives, we are also committed to Diversity, Equity and Inclusion (DEI) and community involvement. These goals aren’t just checkboxes; they’re ingrained in our culture and I’m immensely proud of how our entire team rallies behind them. Not only do they foster a sense of belonging and purpose, but they also cultivate a warm culture of professional excellence.
In addition to our DEI and community involvement goals, another key strategy we’ve implemented, to stay ahead in the rapidly evolving healthcare landscape, is our commitment to developing and commercializing a new solution every year. This strategic initiative keeps us at the forefront of innovation by ensuring that we remain in lockstep with our clients’ evolving strategies, anticipate upcoming regulatory changes and embrace innovation across the marketplace.
By setting and achieving these goals, ProspHire not only stays ahead of the curve but also reinforces our position as a trusted partner in driving positive change within the healthcare industry.
How does ProspHire approach innovation within its consulting services, particularly in an industry as dynamic and regulated as healthcare?
At ProspHire, our approach to innovation within our consulting services, particularly in the dynamic and regulated healthcare industry, is threefold.
Firstly, we prioritize a client-centric approach to innovation. Recognizing that our clients are at the forefront of the industry, experiencing its challenges firsthand, we cultivate deep partnerships with them. By immersing ourselves in our clients’ world, we gain invaluable insights that allow us to collaborate closely in problem-solving and innovation. This hands-on approach enables us to develop tailored solutions that address real-world needs.
Secondly, we foster innovation internally through our own incubation system. Within our Firm, we promote and reward innovation, empowering our team members to submit ideas and concepts. These ideas undergo a rigorous evaluation process through our innovation funnel, where we embrace a culture of ‘fail fast.’ By swiftly iterating and learning from failures, we responsibly deploy our resources towards the most promising innovations.
Thirdly, we stay abreast of regulatory changes and upcoming industry shifts, actively contributing to industry dialogue through white papers and thought leadership. By providing insights and thought-provoking perspectives, we stimulate conversation and promote an innovative approach to problem-solving industry wide.
Through this multifaceted approach, ProspHire remains at the forefront of innovation, continuously striving to deliver cutting-edge solutions that address the evolving needs of the healthcare landscape.
Can you highlight a particularly memorable success story or project that ProspHire has been involved in and what lessons were learned from it?
At ProspHire, our journey has been a continuous learning experience, filled with both peaks and valleys. One of our guiding mantras is ‘We either win, or we learn, we never fail,’ a sentiment prominently displayed on our office wall. This mindset shapes our approach to every endeavor as we strive to build the best healthcare consulting firm in the U.S.
Reflecting on memorable successes, some of the most impactful projects are those from the early stages of our Firm’s evolution. These projects were pivotal in shaping our character, testing our resilience and teaching us invaluable lessons in perseverance. They were not without their challenges – they pushed us to our limits mentally and sometimes physically. Yet, through these experiences, we learned what it truly takes to provide our clients with a white-glove experience while effectively managing the complexities behind the scenes.
These projects taught us the importance of adaptability, innovation and unwavering dedication to our clients’ success. They challenged us to think creatively, pivot swiftly and maintain unwavering professionalism in the face of adversity. While they may have been tough, they yielded immeasurable growth both professionally and personally.
Looking back, these early projects serve as reminders of our journey, reinforcing our commitment to continuous improvement and excellence. They are a testament to our Firm’s resilience and unwavering determination to overcome any obstacle in pursuit of our mission.
In your opinion, what are the most pressing issues or trends shaping the future of healthcare consulting and how is ProspHire positioned to adapt these changes?
In my opinion, one of the most pressing issues in healthcare consulting is the proliferation of fly-by-night solution and product companies that are infiltrating the entire ecosystem. Let me be clear: I’m not advocating for stifling innovation. Innovation is crucial and it’s vital for companies to push boundaries and for clients to explore new products and services. However, the influx of ill-conceived solutions poses a significant threat to the ecosystem. The repercussions of misguided investments can be extensive, leading to costly consequences for patients and members down the line.
At ProspHire, we recognize the gravity of this issue. What sets us apart is our expertise in the domain and our extensive experience in evaluating new solutions and products for their true viability in solving underlying problems. We approach innovation with a discerning eye, carefully assessing whether a solution is sustainable and capable of delivering tangible benefits. This expertise allows us to partner with our clients in navigating the complexities of the evolving landscape, taking calculated steps towards adopting cutting-edge solutions.
As a nimble partner, ProspHire excels in making swift adjustments, anticipating challenges and reacting promptly when things deviate from the expected trajectory. Our ability to pivot quickly and decisively ensures that we remain ahead of the curve, adapting seamlessly to changes in the industry while safeguarding the interests of our clients and the broader healthcare ecosystem.
Given your background in business operations, how do you balance the need for efficiency and effectiveness in delivering consulting services while maintaining high-quality standards?
As someone with a background in business operations, balancing efficiency and effectiveness in delivering consulting services while upholding high-quality standards is at the core of what I do. Throughout the evolution of ProspHire, we’ve focused on building, refining and enhancing systems that facilitate this delicate balance.
Our approach centers around three key pillars: performance management, quality and risk management and our methods and tools. These systems serve as the backbone of our operations, enabling us to consistently deliver exceptional results while optimizing efficiency.
Investing in and maintaining these systems is paramount to our organization’s success. They provide our team with clear guidelines and standards, ensuring that everyone is aligned with the high-quality service we strive to deliver to our clients. Moreover, these systems empower our team members to excel in their professional development, fostering a culture of growth and excellence.
By leveraging these systems, we not only achieve operational efficiency but also uphold our commitment to delivering consulting services of the highest caliber. It’s this dedication to excellence that sets ProspHire apart and enables us to exceed client expectations time and time again.
What advice would you offer to aspiring entrepreneurs or professionals looking to make an impact in the healthcare consulting field?
Firstly, I’ve learned personally the importance of committing fully to your endeavors. Success rarely comes from dipping just one toe in the water; rather, it requires diving in with both feet. I’ve experienced failures when I attempted to pursue ventures on the side of my primary responsibilities. To truly succeed, you must pour your energy, focus and dedication into your goals until you’ve achieved a level of automation and even then, vigilance is key.
Secondly, effective delegation and automation are essential for sustainable growth. As tempting as it may be to have a thumb on everything, it ultimately hinders scalability. Building systems that enable delegation and streamline processes is vital for scalability and efficiency. While challenging, it’s crucial for any venture’s long-term success.
Lastly, I believe that true success lies in leveraging your resources to make a positive impact on others. Resources come in various forms – capital, networks, experience, time – and using them to help others achieve their goals is an integral aspect of any accomplished entrepreneur or professional’s growth journey. Seek opportunities to uplift others and contribute meaningfully to the industry’s advancement.
How does ProspHire build a culture of collaboration, innovation and continuous learning within its team?
At ProspHire, we prioritize building a culture of collaboration, innovation and continuous learning by empowering our team members to take ownership of these aspects. One of our most important strategies has been to decentralize the approach, pushing culture, innovation and learning into the hands of the people rather than enforcing a top-down approach. This approach, which I’m immensely proud of, has proven highly successful over the years.
Unlike many companies that dictate programming and specifics from the top, at ProspHire, we believe in setting the tone from the leadership and then allowing the organization to shape the programming according to its evolving needs. Our culture of collaboration, innovation, education and diversity, equity and inclusion (DEI) is all committee-led, with internal team members rotating at frequencies that best serve those committees.
The Firm provides the necessary resources for each committee to fulfill its plans, resulting in some of the best events, programs, and outcomes for our organization. This collaborative approach not only fosters a sense of ownership and engagement among team members but also drives innovation and continuous improvement.
As a result, ProspHire has been consistently recognized as a best workplace and one of the fastest-growing companies in our industry for many years in a row. By empowering our team members to drive our culture forward, we’ve created an environment where collaboration, innovation and continuous learning thrive, propelling our organization to new heights of success.
Looking ahead, what are your visions or goals for ProspHire in the coming years and how do you plan to achieve them?
As we look ahead, ProspHire has set ambitious goals for the coming years, encompassing typical growth components along with a strong focus on creating exceptional professional opportunities for all our team members. While our growth targets are important, we are equally committed to fostering an environment where every individual can thrive and excel.
Our vision includes not only expanding our footprint and client base but also cultivating a diverse and talented team. We aim to create new avenues for professional development and advancement, providing opportunities for individuals to grow into new roles, become partners, and assume executive leadership positions within the Firm.
To achieve these goals, we will continue to invest in our people, ensuring they have the resources, support and mentorship needed to succeed. As the Firm expands, we will prioritize the growth of our management team, enabling us to provide the leadership and guidance necessary to navigate our growth trajectory effectively.
Furthermore, we are committed to offering many projects that cater to the diverse talents and expertise of our team members. By aligning projects with individual strengths and interests, we can maximize engagement, satisfaction and ultimately, the quality of our deliverables. In summary, our vision for ProspHire in the coming years revolves around both quantitative growth and qualitative development. By creating exceptional opportunities for our team members and fostering a culture of continuous learning and advancement, we are poised to achieve our goals while delivering exceptional value to our clients.
Welcome to the Q&A session with Jaspreet Laungia, the service leader for ProspHire’s Administrative Cost Savings service. Today, organizations are facing the dual challenge of delivering exceptional patient-centered care while optimizing operational efficiencies. Jaspreet brings a wealth of expertise in identifying and addressing inefficiencies in administrative processes, enabling organizations to achieve higher efficiency rates with a leaner team.
What does ProspHire’s Administrative Cost Savings service focus on?
Our Administrative Cost Savings service focuses on enhancing operational efficiency by streamlining processes, analyzing staffing levels and skill mix and reducing inefficiencies ultimately decreasing overall administrative spend while maintaining quality and staying compliant.
How does ProspHire help health plans achieve higher efficiency rates?
We focus on identifying opportunities to streamline processes by either introducing automation, optimizing resource allocation, recommending outsourcing and standardizing operations. This optimization enables organizations to repurpose resources for higher value tasks or increase input altogether, driving up member satisfaction and reducing administrative cost pressures.
What does ProspHire do to assess business processes?
We assess business processes by conducting process, technology and data assessments, comparing resource skill and throughput to industry standards and recommending continuous improvement activities in partnership with stakeholders across a business unit or the entire department.
How do ProspHire’s analyses and recommendations benefit organizations?
Our analyses and recommendations improve resource utilization and help recreate a culture of continuous improvement within organizations, leading to enhanced productivity and cost savings.
What outcomes can organizations expect from ProspHire’s Administrative Cost Savings service?
Organizations can expect improved resource utilization, enhanced efficiencies, cost savings and a culture of continuous improvement that ultimately drives up revenue for health plans while delivering quality to its members.
Welcome to ProspHire’s Soaring to New Health podcast. In this episode, we dive into the transformative power of Data Analytics in Healthcare, joined by Toby George, Co-Founder of Data Ideology. Toby’s expertise sheds light on how data analytics is reshaping healthcare delivery, improving patient outcomes and driving efficiency across the industry.
The Journey of Data Ideology
Data Ideology is a leading firm specializing in Data Analytics solutions for healthcare organizations. Toby explains that their focus lies in helping companies navigate their data and analytics journey, from strategy to execution. They assist organizations in developing a plan and implementing it, particularly aiding those between one and five billion dollars in size that are looking to leverage data as a strategic asset.
Challenges and Solutions in Healthcare Analytics
One of the significant challenges Toby highlights is the slow adoption of advanced technologies like AI and machine learning due to foundational data issues. Many organizations lack a solid data foundation, hindering their ability to adopt these technologies effectively. Data silos, data quality issues and the lack of interoperability pose significant barriers that must be addressed.
The Impact on Patient Outcomes
Despite these challenges, Data Analytics holds immense potential for improving patient outcomes. Toby discusses how predictive analytics can identify potential issues like readmissions, enabling proactive interventions. Machine learning in radiology and natural language processing (NLP) in clinical notes are other areas driving improvements in patient care and satisfaction.
Navigating the Data Journey
For organizations embarking on this data journey, Toby offers valuable advice. Defining a clear vision, understanding the current state and designing a roadmap that avoids overwhelming initiatives are key steps. Cultivating talent, measuring success and iterating are vital for long-term success in data analytics endeavors.
The Future of Healthcare Analytics
Looking ahead, Toby envisions a future where AI, IoT and personalized treatment plans based on data-driven insights play a pivotal role. The Internet of Medical Things (IOMT) presents opportunities for remote monitoring and diagnosis, revolutionizing how healthcare is delivered and experienced.
Data Analytics is not just a tool but a transformative force in healthcare. As organizations embrace data-driven strategies, they stand to enhance patient care, operational efficiency and overall outcomes. With the right approach, partnerships and technologies, the future of healthcare analytics holds immense promise for bettering the lives of patients worldwide.
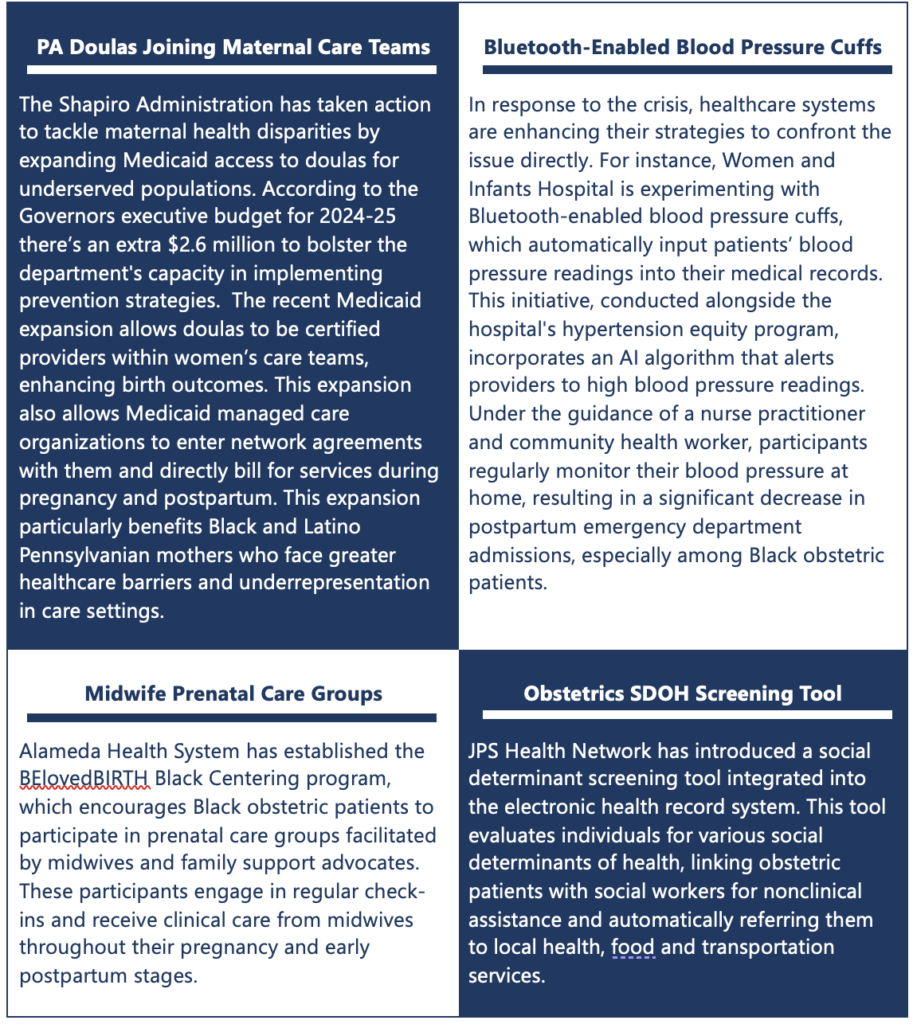
In a nation where the joy of childbirth should be universally celebrated, the harsh reality persists as maternal mortality rates continue to rise and disproportionately impact black women. The Centers for Disease Control and Prevention (CDC) reported 32.9 deaths per 100,000 live births in 2021, highlighting a concerning trend from 20.1 in 2019 and 23.8 in 2020. This disparity underscores systemic healthcare inequalities. However, amidst these challenges, hope emerges with a transformative initiative led by the Centers for Medicare and Medicaid Services (CMS).
As per a report from Modern Healthcare, CMS introduced a pioneering initiative in 2023 allocating $17 million over a decade to reshape maternal healthcare, covering both physical childbirth aspects and mental and social needs. With Medicaid funding 40% of childbirths nationally, these grants have transformative potential. The initiative aims to revolutionize maternal care by promoting collaboration among healthcare providers and increasing access to complementary services like midwives and doulas. Particularly focused on underserved rural and low-income communities, it aims to establish birth centers and minimize unnecessary cesarean sections.
Critical to this endeavor is the integration of screening programs for Social Determinants of Health, nutrition, housing, substance use and the facilitation of connections to community-based resources. States accepting CMS funds are mandated to develop health equity plans and extend Medicaid coverage for a full year postpartum, recognizing the significance of continued care beyond childbirth.
Strategies to Improve Maternal Health Equity
Navigating the complexities of systemic change is crucial as the United States grapples with a concerning increase in maternal mortality rates, particularly affecting black women. CMS’s Medicaid maternal health grants mark a pivotal step towards achieving equity in maternal care. However, sustained efforts, driven by a commitment to justice and inclusivity, are essential to ensure every mother receives the care and support she deserves, regardless of race or socioeconomic status.
At ProspHire, we specialize in driving impactful change across healthcare. Our teams closely monitor the Medicaid landscape, shaping quality enhancements and financial progress. With our deep industry expertise and focus on building crucial connections with underserved populations, we are positioned at the forefront of the field. As you explore avenues to integrate maternal health care and SDOH management, connect with us.
ProspHire proudly welcomes Tim Calhoun as our newest Managing Director, bringing with him over two decades of invaluable healthcare experience. Formerly from Ernst & Young (EY), Tim has been instrumental in serving healthcare clients across commercial, nonprofit and governmental sectors. His decision to join ProspHire underscores our commitment to excellence in healthcare consulting. Tim’s wealth of knowledge will undoubtedly elevate our client offerings and our standing as industry leaders. Today, we are diving into Tim’s motivations for choosing ProspHire, his strategic vision for leveraging his healthcare experience to drive growth and his unwavering dedication to delivering exceptional project outcomes for our clients.
Can you share more about your background and what led you to join ProspHire as Managing Director?
I started out in accounting and auditing in both manufacturing and financial services industries; my undergraduate degree was in accounting from Penn State. I obtained my Executive MBA from Pitt and coming out of graduate school I was drawn to consulting because of the variety of opportunities and the challenge of working with clients on key initiatives that are important to them and their stakeholders. For most of my career, I have been involved with clients from regulated industries, financial services and utilities but making the decision to focus on healthcare required me to double down on understanding the industry and figuring out how to apply my earlier learnings and experience to a new space – what I refer to as pivoting.
What attracted me to ProspHire was the 100% focus on healthcare and when I arrived, it was the caliber of the people and their knowledge and experience that reinforced that I made the right decision. The entrepreneurial spirit, the culture and the ability to make quick decisions were also attractive.
Up until joining ProspHire, I spent my consulting career with global firms. In 2010, I had the opportunity to help rebuild a health practice, which I enjoyed a great deal. Because of that experience, I knew that if I were to make a change, I wanted to change it up. I found that with ProspHire – a focus and energy on healthcare, an entrepreneurial environment and an opportunity to have impact on building the next generation of leadership.
How do you envision leveraging your experience to help drive the strategic vision of ProspHire?
There is such a solid foundation and forward momentum to build upon. One of the key reasons for making the move to ProspHire was the opportunity to contribute to defining the future direction – understanding the strengths of the firm, envision the direction of our industry and how we can best help our clients and our teams achieve success. The leadership team is dedicated to our clients’ success, prioritizing support for our internal teams and leveraging our collective experiences to develop best practices for the future. I have had the opportunity in my previous role to gain experience in envisioning how we can help our clients and putting that into action. I want to “capture lightning in the bottle” again.
What are some key challenges you anticipate facing in your new role and how do you plan to address them?
There are internal and external challenges. From an internal perspective, I have been with several firms. While there are common threads in consulting, each firm has their own focus and community culture. I need to take the time to learn about these and make sure that I do not undermine the culture and community that has made ProspHire successful. That means I need to listen more than talk… for those who know me, that is a tall order. Listening is also a key requirement to contributing to the refinement of the strategic vision.
Externally, re-engaging with client relationships, building new relationships and educating them on what ProspHire offers. I am anxious to contribute and be incremental to our success. Developing new relationships and maintaining those who already know me is something that I have had to do for some time so it is really understanding what we can offer today in addressing our client’s challenges and collaborate with clients to meet their needs and timelines.
Could you elaborate on your experience collaborating with health plans and state health agencies to streamline administrative processes and drive transformative initiatives?
One of the first opportunities that I had in getting involved with health care was my involvement with a US-based performance metrics study that examined and compared insurers performance across the entire process value chain, including costs, process, quality, technology and staffing. It gave me a solid foundation in understanding how top performing plans operate, as well as a keen understanding of how up- and down-stream processes impact each other.
I was also fortunate to get a great deal of insights in how state agencies and health plans worked and interacted with each other in the Medicaid space – both in the implementation of their core platforms but also in understanding how to communicate with the states and CMS.
On the Medicare book, it is about understanding the regulations and the impact to core clinical and administrative operations. A lot of that comes from just getting involved with those initiatives. This experience was tested when helping an insurer get its Medicare Advantage book of business out of CMS sanctions. Given the growth of Medicare and Medicaid, I am fortunate to have gotten involved in them early in my career.
What are your priorities in terms of expanding ProspHire’s client base and enhancing service offerings?
I am looking forward to learning more about our existing service offerings and solutions so that I can articulate to our current clients and future clients what we do exceptionally well. That is really the first order of business and everyone at ProspHire has been so good at educating me.
My initial thoughts on expansion are focusing on clients’ needs related to doing more with less while navigating the current uncertainties of the marketplace – economic, upcoming election, increased regulations and customer trust. This implies the need for strong core operations and administrative costs efficiencies across commercial, Medicare and Medicaid. Insurers need to take the opportunity to weather these challenges and come out well positioned to optimize expense management, technology to improve operation workflows and maintain quality and affordable care.
How do you build collaboration and innovation within the team to ensure continued success and growth?
I see my job as learning what is important to each of our team members to be successful and how they define success. It is going to be different for each of us. The trick becomes how do we align that with what is important to our client’s success. Sharing and collaborating on opportunities and taking the approach of pulling in the right set of team members to make the client successful will be key.
Can you provide insight into specific areas with healthcare consulting that you believe holds the most potential for growth and development in the coming years?
Medicare and Medicaid are lines of business that will continue to grow; it just so happens, processes and regulations will create the greatest needs because of the regulatory complexity. I do believe that ProspHire is positioned to help our clients meet those needs, along with supplemental benefits – the Firm has a very strong and growing dental operations solution.
We are also seeing growth potential for our “payvider” clients and believe that this segment will continue to grow and will have unique opportunities where we can support them.
What role do you see technology playing in shaping the future of healthcare consulting and how do you help to incorporate technology advancements into the firm’s strategies?
Technology serves as a driving force for innovation and transformation in navigating the complex healthcare landscape. We need to help our clients think through how to leverage technology tools and solutions that address today’s healthcare challenges.
In the near term, I see insurers focusing technology initiatives in the areas of improving workflow quality and timeliness in clinical and administrative operations, such as Appeals and Grievances, Provider Network data, Stars and Quality measures. These areas allow insurers to quickly address member and provider needs and regulatory changes. And of course, we cannot talk about technology without mentioning how advanced analytics and Artificial Intelligence (AI) will impact healthcare. The value of AI will come in helping to identify clinical and administrative options. We still are learning how to use AI and what are the limits of its capabilities. My thinking is that healthcare should be using this technology in identifying potential options in care and claims management but human decision-making is still required in executing.
I am excited to help think through how we incorporate technological advancements into our solutions and strategies that focus on how we help our clients transform.
How do you plan to uphold ProspHire’s commitment to providing unparalleled expertise and leadership to its clients and what measures will you take to ensure client satisfaction and success?
By listening to what our clients’ needs are and what it means to them personally and professionally. It is not enough that we help the client solve their challenges, but we want to help them to be successful too. We work in an industry where there is not much differentiation in what we do. Our clients need to know us as someone who they can call to help them solve a critical need.
Welcome to Season Two of ProspHire’s Soaring to New Health podcast! In this episode, we delve into the critical impact of Social Determinants of Health (SDOH) on our communities, particularly focusing on housing and its implications for the well-being of children and families. Joining us today are two distinguished guests: Stephanie Meyer from the Pennsylvania Department of Human Services and Chris Watts, the CEO of the Boys and Girls Clubs of Western Pennsylvania.
Chris Watts shares insights into the Boys and Girls Clubs’ mission, serving over 7,500 kids annually in Western Pennsylvania. Their programs focus on providing safe environments, academic support, character development, healthy lifestyles and career readiness to help children reach their full potential.
Stephanie Meyer highlights the role of the Pennsylvania Department of Human Services in supporting over 3 million Pennsylvanians through various programs, including Medicaid, nutrition assistance and housing initiatives. The department’s focus on addressing housing instability and providing critical resources during the pandemic reflects their commitment to a thriving Pennsylvania for all.
Tackling Barriers: The conversation shifts to addressing housing barriers, with Stephanie discussing initiatives like the Emergency Rental Assistance Program and efforts to increase access to affordable housing. Chris Watts emphasizes the Boys and Girls Clubs’ commitment to reducing barriers for families, including transportation and paperwork processes, to ensure all children have access to quality programs.
The Impact of Social Determinants: Both Stephanie and Chris emphasize the tangible impact of Social Determinants of Health, such as homelessness and housing instability, on children and families. They paint a vivid picture of the challenges faced by those experiencing housing insecurity and underscore the need for collaborative efforts to address these disparities.
Investing in Quality and Access: Both community leaders highlight the importance of investing in quality childcare and early learning programs. Stephanie praises the Boys and Girls Clubs’ commitment to quality, as evidenced by their high accreditation rating, while Chris emphasizes the need to ensure access to high-quality programs for all children, regardless of their circumstances.
It’s evident that addressing Social Determinants of Health requires a multifaceted approach involving government agencies, community organizations and stakeholders. By working together and investing in quality programs and resources, we can create a healthier and more equitable future for our communities. To learn more about how you can get involved, listen to the entire episode here: Listen to the Soaring to New Health Series | ProspHire
The beginning of the calendar year means it is HEDIS/Medical Record Review season and within this timeframe; everyday matters, so make them count. With approximately a month left, health plans need to leverage their strategic provider partnerships and utilize data reporting and tracking to optimize opportunities for quality improvement (QI) and ultimately achieve their year-end Stars’ goal.
Leveraging provider partnerships: Now is the time to lean in on your plans’ relationship with providers who care for your members. Utilizing your previously developed provider repository, accessing provider group Electronic Medical Records (EMRs), and knowing when to escalate in areas needing additional support is key.
Data reporting and tracking: Real-time data updates regarding chart chase status, measure-level gap analysis/forecasting and identifying key opportunities for broad chart closure efforts are critical to ensuring a successful close-out to Hybrid season.
SY2026 Strategic Plan and Execution
As we enter a new Stars Year, it is critical that your plan is poised for success by setting clear and achievable goals. This year presents the opportunity to innovate and refine your plan’s approach, particularly with new interventions targeting both identified priorities and newly introduced measures. As we navigate the ever-evolving Stars landscape, it is key to maintain alignment across all areas of the organization to effectively adapt to industry changes and emerging trends. By fostering collaboration and strategic alignment, your plan can maximize its potential, achieve the goals set forward and make a meaningful impact on the health of your members.
Ensure your goals are set: Conduct goal setting activities to achieve your contract-level goals and establish priority measures that will have significant impact on your plans performance if the goals are achieved.
Develop new interventions for priority measures: Plans must look ahead and continue to be innovative with interventions, relying on what got you here will not get you to where you want. Develop key strategies around the priority measures to ensure continuous improvement is driven forward.
Alignment across the organization of industry changes for SY2026: Plans must understand how the industry is changing every year in Stars. With the weighting shifting away from member experience, success in HEDIS will be more necessary to drive a plan’s performance. Key changes for this SY are outlined below:
Addition of Kidney Health for Patients with Diabetes (1x weight)
Colorectal Cancer Screening removed from Hybrid Reporting – moved to Electronic Clinical Data Systems (ECDS)
Introduction of Health Equity Index – monitoring applicable HEDIS measures for Social Risk Factors
At ProspHire, we continue to partner with health plans, to offer insights, analysis and execution strategies to improve Star ratings. Do you need support developing the right SY2026 execution strategy? Let’s have a conversation.