Medicare Advantage Value-Based Insurance Design Model
On April 5th, 2023, CMS announced the extension of the Value-Based Insurance Design (VBID) Model.
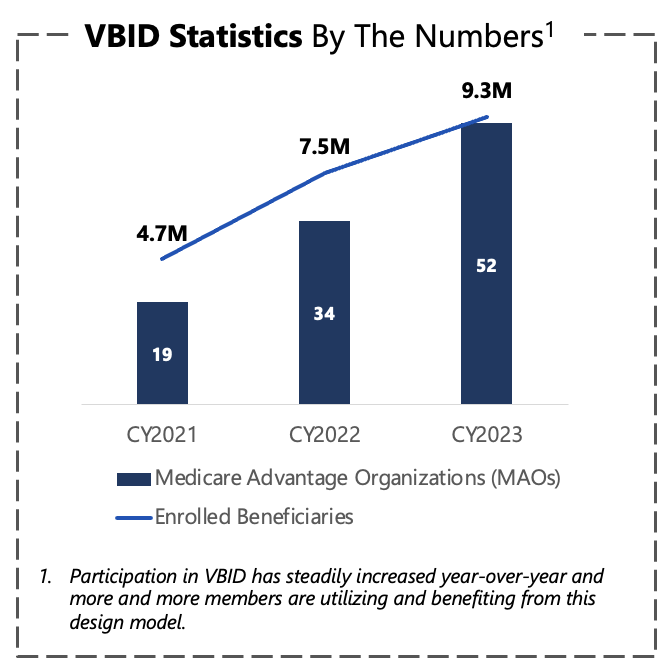
The VBID Model aims to increase use of high value services, while increasing flexibility of participating Medicare Advantage organizations to provide targeted supplemental benefits to meet the needs of their enrolled population.
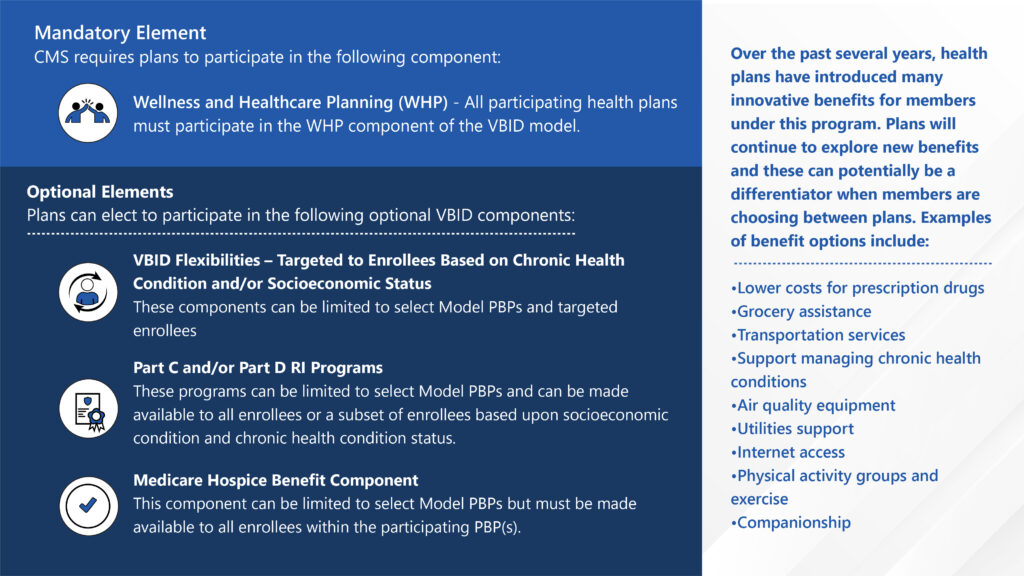
Starting in calendar year (CY) 2024, the VBID Model will be testing several model components, some new and some existing. Participating health plans will be required to engage in the Wellness and Health Care Planning component of the VBID Model in CY2024 in addition to testing one or more of the other interventions in CY2024. These model components include:
Wellness and Health Care Planning (WHP)
VBID Flexibilities (Model PBPs’ select enrollees targeted by condition, socioeconomic status or a combination of both)
Part C and Part D Rewards and Incentives (RI) Programs
Hospice Benefit Component
VBID 101: What You Need to Know About VBID
Key VBID Facts:
Members must earn or redeem rewards and/or incentives within the contract year in which the program has been implemented. Gift cards can be considered an acceptable form of reward or incentive so long as they are not redeemable for cash by the member.
Medicare Advantage Organizations may include information about the VBID program in marketing materials, so long as those materials are provided equitably to all current and prospective enrollees without discrimination.
The VBID program cannot be used to specifically target populations as potential enrollees.
Reporting
Participating organizations must report supplemental benefit utilization to CMS twice annually. Included in this reporting requirement under the Flexibilities component are supplemental benefits for food and nutritional insecurity, transportation barriers and living supports.
Reporting Requirements: (From CMS MA Reporting Technical Manual)
15.1 Do you have a Rewards and Incentives Program(s)? (“Yes” or “no” only)
15.2 What health related services and/or activities are included in the program?
15.3 What reward(s) may enrollees earn for participation?
15.4 How do you calculate the value of the reward?
15.5 How do you track enrollee participation in the program?
15.6 How many enrollees are currently enrolled in the program?
15.7 How many rewards have been awarded so far?
Core Program Elements
The core elements of the VBID Model cover health care planning, supplemental benefit provision, rewards and incentives and extra hospice support. Health plans can apply to tailor the optional elements based on CMS provisions to best meet member needs.
Health Equity Plan A New VBID Element in 2024
Starting with the 2024 VBID Model, each plan is required to submit a VBID Health Equity Plan. This contains the health plan’s strategy to advance health equity through participation in the VBID Model.
Key Elements:
Health plans must identify priority populations and screening tools that will be used to capture disparities and health-related social needs.
Health plans must define the actions that they will take to address the identified disparities, overcome potential barriers and refer members to appropriate support services.
Health plans must present information on metrics and monitoring approach for the strategies presented in the Health Equity Plan.
Finally, health plans must explain their education and engagement strategies for members as well as providers, caregivers and broader communities.
Preparing for Success
Participating health plans should expect to receive provisional approval on their CY2024 Medicare Advantage VBID applications in Mid-May.
Is your plan equipped to implement your VBID model in 2024? Medicare Advantage Organizations must consider their supplemental benefit vendor readiness, strengthening their quality and population health programs and ensuring medical management preparation for the new VBID program year.
ProspHire’s Medicare experts are prepared to support your organization in planning for VBID success.
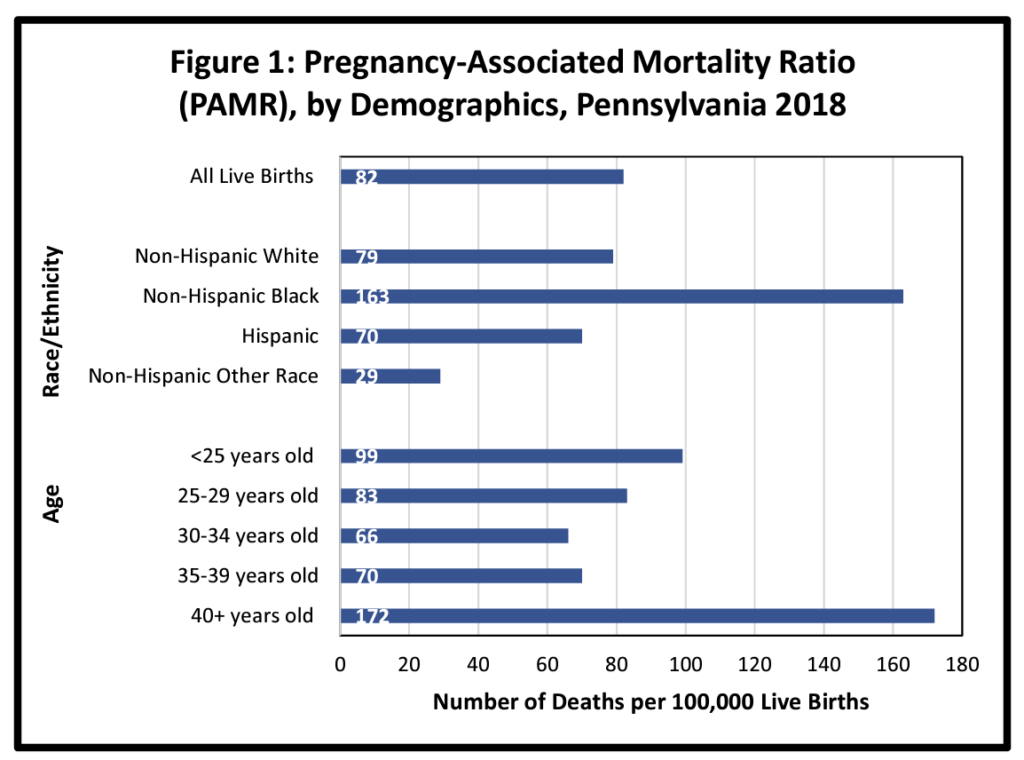
Among developed countries, the United States falls behind in maternal health outcomes. According to the Commonwealth Fund, in 2020 the United States maternal mortality rate was 24 deaths per 100,000 live births which is more than three times higher than the majority of other high-income countries. ProspHire’s home state of Pennsylvania is no exception. Disaggregating health data within the United States by race reveals a significant difference in outcomes. According to Penn Medicine, black women are three times more likely to die from pregnancy-related complications than white women in the United States. These disparities are further evident in Pittsburgh, the location of ProspHire’s headquarters, which was identified as having the highest maternal mortality rate for black women amongst all United States cities (Pittsburgh NPR).
For health plans and providers seeking to address these shortcomings in maternal health equity, what can be done?
The Role of SDOH in Addressing Health Inequities
Healthcare industry experts have identified social determinants of health (SDOH) as useful indicators that provide insight into patients’ quality of life and health. SDOH variables include patients’ socioeconomic conditions, and the extent to which they have a disparate impact on health outcomes. Health plans can identify at-risk members within a given population by utilizing available data which provides a broad consensus on the role of SDOH in maternal health inequities. One resource underutilized by health plans is community-based organizations (CBOs), broadly defined as NGOs, nonprofits and community healthcare facilities. The Affordable Care Act (ACA) provides incentives for partnerships between health plans and CBOs which have proved helpful in addressing social determinants of health.
Health Plan-CBO Partnerships and Addressing Maternal HealthEquity
Health plan-CBO partnerships are especially promising in addressing maternal health equity because they are directly familiarized with addressing community and family-level drivers of inequality1. Once criteria have been determined, such a partnership can work together to take the necessary steps to help at-risk patients.
Fostering relationships between health plans and CBO’s can assist in better identifying target population needs. Reputable CBOs generally cultivate a high level of trust and rapport within their communities. The following are a few example areas where CBOs can assist with solutions to achieve maternal health equity: expanding prenatal care, conducting cultural sensitivity trainings for medical staff, collecting survey data, health education, providing childcare, and hosting prenatal education classes.
Illustrating Success
When looking for a best-case example of a CBO addressing maternal health equity, one can look to ProspHire’s office location in the greater Philadelphia area. The Maternity Care Coalition in southeastern Pennsylvania partners with neighborhoods with high rates of poverty, infant mortality and health disparities.
The Community-Based Health Care Program, funded by the Department of Health, provides funding to existing community-based care facilities to expand or build upon existing services. The Commonwealth Fund has identified the following community-based models which health systems can invest in to improve the patient experience and health outcomes for vulnerable patients:
Community-Based Doulas
Midwifery Services
Group Prenatal Care
Non-Hospital Based Birthing Centers
For health plans seeking to adopt evidence-based models of care to improve maternal health outcomes, they may find it beneficial to partner with these existing services.
Important Considerations
Basic criteria which are important to assess when identifying potential community partners include: how they operate in the local area, their reach and expertise. To allow these partnerships to reach their full potential, it is important to identify a general set of challenges that come with health plan-CBO partnerships. According to the Center for Health Strategies, some important considerations include:
Establishing sustainable funding models
Selecting and collecting partnership impact metrics
Sharing patient-level data
How ProspHire Can Help
Health plans can utilize ProspHire to help identify SDOH drivers for maternal health, pinpoint areas of greatest need and establish criteria for potential CBO partnerships based on the unique needs of your service area and most vulnerable patient populations. From a population assessment and recommendation to implementation, our work is focused on addressing health disparities across communities of greatest need and improving equitable care and outcomes.
Did you know April 22nd is National Prescription Drug Take Back Day? Sponsored by the Drug Enforcement Administration (DEA), National Prescription Drug Take Back Day promotes medication safety and disposal in our communities across the country. Unnecessary prescription drugs, including opioids, can be misused, or abused by individuals prescribed the medications or unregulated members of the community with access to the medication supply. Encouraging the public to remove unnecessary medications from their homes is important to the public health and safety of Americans. This annual event can prevent prescription medication misuse and avoid potential opioid addiction.
The disposal window for National Prescription Drug Take Back Day is 10 AM to 2 PM.
The DEA Prescription Drug Take Back Day website has resources to find collection sites in your area. The Collection Site Locator feature allows you to search for public collection sites by zip code, county, city or state levels. Unused and unwanted prescription medications will be accepted at more than 4,000 drop-off locations across the country. Be sure to remove any personal identifiers, such as name and date of birth found on your prescription bottles, from any packaging prior to medication disposal. You can find this tool and other information regarding National Prescription Drug Take Back Day here.
Why is National Prescription Drug Take Back Day Important?
According to a 2015 article in the Journal of Environmental Management, the United States produces the most medical waste among all world countries, accounting for more than 3.5 million tons annually. Many households across the country have unused medications spread across different rooms and storage containers. Some medication treatments become outdated due to advancements in disease treatment, changing of prescription medications for improved disease state management and general discontinuation of medication therapy. Throwing unused medications into the regular trash at home can result in environmental harm, pollution and even accidental death if ingested. The DEA even accepts vaping devices and cartridges at these sites for safe disposal. More than 324 tons of unwanted medications were collected across the country at the October, 2022 National Prescription Drug Take Back Day.
How Can ProspHire Help?
At ProspHire, we can assist your health plan with decreasing medication waste through the implementation of significant services focused on medication utilization. Our team of clinical experts can analyze your data and identify medication use patterns to provide waste reduction strategies with the opportunity for prescription medication deprescribing.
The 2024 Medicare Advantage and Part D Final Rule has been released.
On April 5, 2023, CMS released the highly anticipated final rule. This comes just after CMS released the 2024 Medicare Advantage Capitation Rates, Part C and Part D Payment policies on March 31, 2023.
It is essential that plans begin preparing for these impacts now. It is critical that stakeholders understand these changes to methodology, calculations and measures. Developing strategies for these key changes will enable your program to continue to be forward-thinking and positioned for future success.
ProspHire’s team of Medicare experts have reviewed the final rule for insights relevant to our Medicare Advantage and Part D partners. Below, we highlight several key changes detailed in the final rule.
Here’s what you need to know about the latest final rule changes from CMS relevant to Medicare Advantage Health Plans.
Summary of Final Changes | Risk Adjustment Impacts
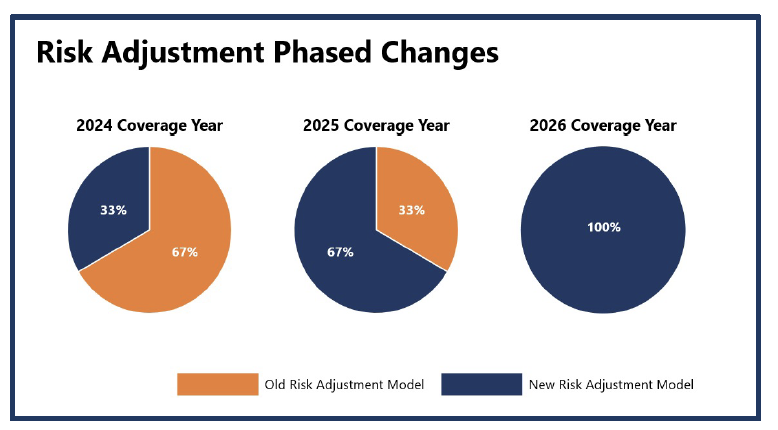
Overview: Within the CMS Final Rate Announcement, CMS has proposed changes to the Part C Risk Adjustment Model to eliminate coding variation and improve payment consistencies to MA plans year over year. Many commenters requested a phased-in approach illustrated on the right, as there will be large process changes and needed education; this approach has been utilized for model updates in previous years.
Old Risk Adjustment Model: Utilization of the ICD-9 code classification system and related HCC Codes.
New Risk Adjustment Model: Utilization of the ICD-10 code classification system, clinically revised HCC codes and an increase in the number of HCC codes (86 →115).
Additional Detail of New Risk Adjustment Model:
The HCC Model was last updated two years ago with FFS claims from program years 2014 and 2015. The revised HCC model will use diagnosis codes from 2018 and expenditures from 2019.
The new model revises the average per-capita expenditure model to include denominators from 2015 through 2022.
The updated risk model implements frailty factors to account for the PACE and FIDE SNP populations.
With this adjustment, plans should begin to evaluate their current risk coding processes to ensure the new risk adjustment model is accurately implemented and downstream revenue impacts are minimized. It is imperative that plans begin to:
Enhance education and tools to support provider partners
Ensure clear coding specifications and processes are implemented across the organization
Establish a governance process in 2024 to monitor the implementation of the model and continue to improve processes
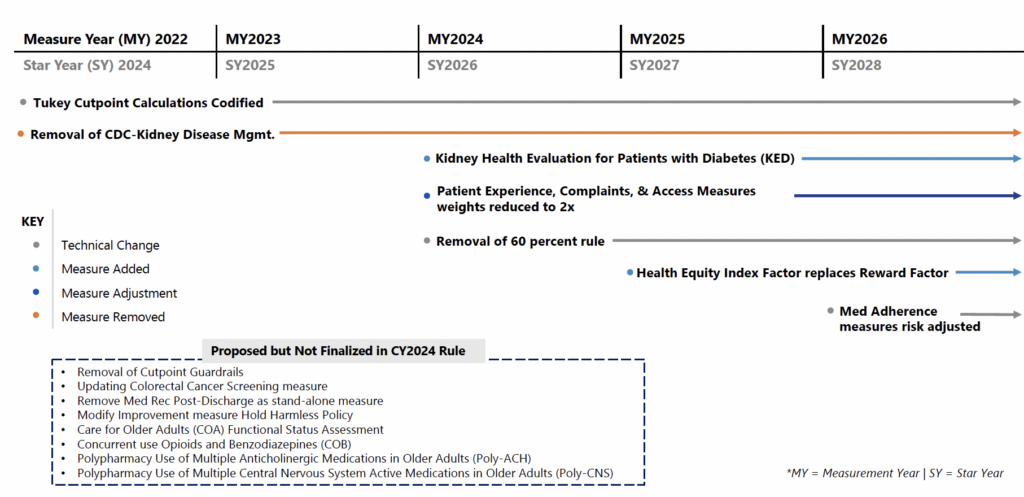
Final Rule Changes | Stars Timeline Impact
*MA Stars changes will begin in MY2022 (SY2024), with tiered rollout continuing through MY2026 (SY2028).
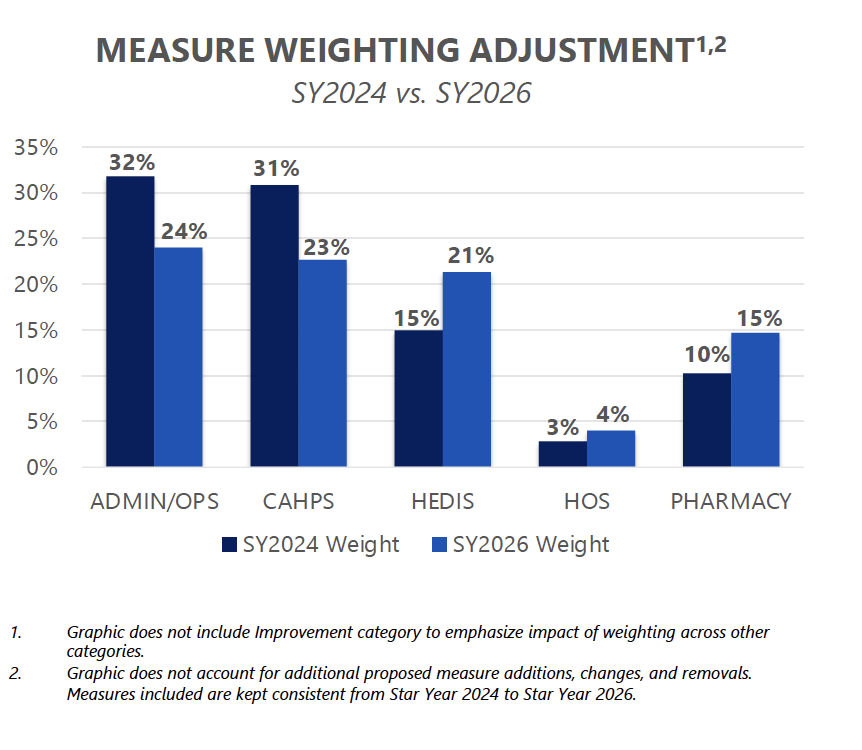
Final Rule Changes |Stars Measure Weighting Shift
Key Insights: The CMS final rule will reduce the weight of the member experience, complaints, and access measures by half. Previously, these measures were weighted at 4x, but for SY2026 these measures will be weighted as a 2x. Reducing the weighting will better align the patient experience/complaints and access measures more closely with other domains. Plans should continue to focus interventions around listening to the voice of the member given the important link between patient experience, retention, medication adherence and other health outcomes.
Final Rule Changes |Replace Reward Factor with HEI
CMS is proposing to replace the reward factor with a health equity index (HEI) reward for the 2027 Star Ratings to incentivize plans to focus on improving care for enrollees with social risk factors (SRF).
Reward contracts for obtaining high measure-level scores for a subset of enrollees with specified Social Risk Factors (SRFs). The HEI reward is intended to improve health equity by incentivizing MA, cost and PDP contracts to perform well among enrollees with specified SRFs. The HEI is designed to work in conjunction with the current CAI (the measure of a contract’s performance relative to its peers) rather than replace it. CMS intends to use the HEI to assist plan sponsors in better identifying and addressing disparities in care provided to members with SRFs. CMS has the ultimate goal of reaching equity in the quality of care provided to enrollees with SRFs. The HEI reward would be calculated using data collected or used for the 2026- and 2027-Star Ratings (2024 and 2025 measurement years) and would initially include LIS/DE or having a disability as the group of SRFs used to calculate the HEI. The regulatory change from CMS involves five proposed steps that CMS would take to analyze the measure-level scores for each contract and roll up to the HEI scores to assess when an adjustment is available for a contract’s ratings.
These steps involve:
A modeling approach to calculate the scores for the subset of enrollees with SRFs of interest included in the HEI
Adjusting measures that are case-mix adjusted in the Star Ratings
Using inclusion criteria for measures to be rolled into the HEI score for a specific contract
The distribution of contract performance on each eligible measure among enrollees with the specified SRFs would be calculated and separated into thirds to assign a HEI score to a contract.
Stay tuned for more information on the HEI calculation and potential opportunities to collaborate with Social Determinant of Health champions at your health plan.
Summary of Final Changes | Sales and Marketing
The final rule aims to safeguard Medicare beneficiaries from misleading marketing and aims to provide them with accurate and necessary information to make informed decisions about coverage options. To address this, CMS includes the following provisions for Medicare Advantage sales and marketing activities:
Television advertisements, such as commercials, must identify a plan name stated at the same pace as the contact information.
Marketing content that causes confusion or misleads beneficiaries is prohibited. This includes the misleading use of the CMS or Medicare names and logos, advertising benefits not available in the beneficiary’s service area and use of superlatives (e.g. “best”) without current source documentation references.
CMS will hold plans accountable for stricter oversight of agents and brokers by requiring plans to monitor and report non-compliance to CMS.
In addition, the final rule includes guidelines on agent requirements, restrictions and permissible activities. Some changes include:
Brokers and agents must cover CMS-specified information when meeting with a prospective member and these calls must be recorded.
Scope of Appointment cards cannot be collected at educational events but Business Reply Cards may be made available to attendees by brokers.
Agents must identify all Medicare Advantage or Part D organizations they sell on their marketing materials.
Agents can re-contact beneficiaries to discuss plan options for up to twelve months.
Summary of Final Changes |Behavioral Health
The final rule identifies several behavioral health changes related to network management, access and adequacy, as well as clinical management and coordination, with the stated aim to increase parity between physical and behavioral health services for enrollees in the Medicare Advantage program.
From a network lens, the Final rule initiates the inclusion of Clinical Psychologists and Licensed Clinical Social Workers in network adequacy requirements. CMS also expands the 10-percentage telehealth credit to reach more behavioral health providers by extending eligibility to Clinical Psychologists and Licensed Clinical Social Workers. Further, the final rule requires health plans to notify members when their behavioral health clinician is removed from the plan’s network during the plan year. The final rule also includes behavioral health specialties in proposed future standards for appointment wait times.
Additionally, clinical teams can expect changes in behavioral health management and coordination with the CY2024 Final Rule. CMS requires plans to exclude emergency behavioral health services from prior authorization. The Final Rule also expects health plans to instate care coordination programs incorporating behavioral health services.
Overall, health plans should expect an increase in their network management responsibilities to integrate these broader behavioral health requirements. Clinical teams should prepare to meet CMS standards for care coordination services for behavioral health and invest in establishing programs for this population per the Final Rule. Utilization management programs must ensure that their prior authorization policies and systems enable the exclusion of emergency behavioral health services from prior authorization requirements.
ProspHire’s Integrated Clinical Solutions experts are prepared to support your health plan in developing clinical transformation plans to prepare for these changes. Our team members are prepared to help your organization with the change management to ensure processes meet CMS guidelines.
Is your health plan ready to react to these changes in CY2024 and beyond?
ProspHire is ready to partner with your health plan to prepare and plan for these changes to the Medicare program.
Did you know? April is Medicaid Awareness Month.
Medicaid Matters. It’s a lifeline for millions of Americans and is especially critical as the nation responds to the pandemic, providing key funding for hospitals and helping patients get the support they need.
Medicaid is the country’s most extensive health care program specifically designed to meet the needs of low-income individuals who have disproportionate medical needs and health challenges. Medicaid provides high-quality, affordable coverage to nearly 80 million low-income individuals and families, including 10 million people with disabilities. The program is the main source of long-term care coverage for millions of older adults and, along with the Children’s Health Insurance Program (CHIP), provides access to care for over 40 million children.
Why is Medicaid Awareness Month important?
One of the key goals of Medicaid Awareness Month is to raise understanding about the program and the services it provides. Many people may not realize that they are eligible for Medicaid or may not be aware of the range of services that are covered. By increasing awareness, we can help ensure that more people are able to access the care they need to stay healthy.
It has been proven that Medicaid expansion efforts have increased access to care, improved financial security and led to better health outcomes. The Medicaid expansion has played a pivotal role in reducing racial disparities in obtaining healthcare access.
The Public Health Emergency (PHE) is set to expire on May 11, 2023. The PHE has been in place since 2020 due to the Covid-19 pandemic. During this time, Medicaid/CHIP enrollment grew by more than 20 million. The PHE gave the federal government flexibility to waive or modify Medicaid and CHIP programs. Starting this Spring, States will begin the process to determine who will no longer be eligible for coverage. It is estimated that up to 15 million Medicaid and CHIP enrollees will lose coverage over the next 12 months.
It is expected that up to a third of those losing coverage will turn to Health Insurance Exchange Marketplaces. Consumers who have lost coverage during the Medicaid unwinding process will be eligible to apply for immediate coverage through a Special Enrollment Period (SEP). While many Issuers are scrambling to replace lost Medicaid revenue, ACA Marketplaces are a strategic place to look.
How Can ProspHire Help?
At ProspHire, our approach is to gain a fundamental understanding of your existing business, operations and goals and then develop the best strategy to achieve your ACA goals quickly and effectively. We can assist your health plan with conducting an assessment and instituting change management throughout the Medicaid unwinding’s and help to ensure ACA and other products are optimized to secure continued coverage for those losing Medicaid.
Imagine a world in which every person, from infants to seniors, can achieve and maintain their highest level of health. This goal is health equity and while it should be a societal norm, many obstacles make it difficult to reach.
These barriers lead to health disparities, which are differences in the health statuses of varying groups of people. Health disparities are avoidable distinctions in the burden of illness, injury, disease, violence or chances to attain good health that socially disadvantaged groups face.
Health inequities are linked closely to the disproportionate allocation of social, economic and environmental resources. However, health professionals can work to address these disparities by understanding why social health determinants are important and what support services can help.
What Are 5 Social Determinants of Health?
Social determinants of health are the nonmedical circumstances in our environment that impact our well-being. Factors present in the places where we are born, live, play, learn, work, and age can profoundly influence our overall quality of life.
Social determinants of health also cover a broader set of systems and forces that shape daily life. These health determinants can comprise economic policies, development agendas, social and cultural norms, racism, climate change and politics.
To understand social determinants of health, consider the following examples:
Safe housing, transportation and neighborhoods
Discrimination, racism and violence
Education, job opportunities and income
Access to nutritious foods and opportunities for physical exercise
Clean air and water
Language and literacy skills
Professionals group the social determinants of health into five domains, which we’ll explore below.
1. Economic Stability
Economic stability means having enough secure, reliable income to meet your fundamental needs. Being economically stable can help you achieve a better quality of life by allowing you to access essential resources for your health and well-being.
Factors that influence economic stability include:
Affordable housing
Employment that provides a living wage
Employment benefits, like worker protections, paid sick leave and child care
Reliable transportation
It’s crucial to address economic instability as a social determinant of health because daily challenges surrounding unemployment, poverty, housing and food insecurity can elevate the risk of poor health outcomes for vulnerable populations.
2. Education Access and Quality
Education equips people with the tools they need to live fulfilling lives, thrive personally and contribute to their communities. Moreover, an educated person is more likely to access elements that contribute to their well-being, like quality healthcare, jobs that pay a living wage and safe living environments.
People with access to a good education tend to stay healthier throughout their lives than those without. Education gives people the opportunity for upward mobility, placing them in the financial circumstances necessary to access quality healthcare and support services.
People with low education levels contend with unemployment and low income, which are associated with poorer health. Data indicates that people of lower socioeconomic status experience more health problems like obesity, asthma, diabetes and heart disease than people of higher socioeconomic status.
Finally, having a college education helps job seekers obtain higher-paying work that poses fewer safety risks.
Ultimately, people with higher levels of education have more means to afford things that promote their health, like quality housing in toxin-free environments and expert primary care physicians trained in the most successful techniques.
3. Healthcare Access and Quality
Access to quality healthcare means services like the prevention, diagnosis, treatment and management of diseases, illnesses, disorders and other health-impacting conditions are readily available to you. These healthcare services must also be affordable and convenient.
Unfortunately, many people encounter obstacles that make it challenging to obtain health care services, which may increase the risk of poor health outcomes and disparities. Such barriers include a lack of health insurance, inadequate healthcare resources and limited access to transportation.
Little or no health insurance coverage significantly hinders healthcare access. High costs may cause people to put off necessary medical treatment or avoid it altogether. Lower-income families often go without insurance and minority groups constitute over half of the uninsured population.
Inadequate health insurance coverage can adversely impact a person’s health. Adults without insurance are less likely to receive preventive care for chronic conditions like diabetes, cancer and heart disease. Likewise, uninsured children are less likely to get treated for conditions like asthma or receive critical services like dental care, immunizations and well-child visits.
Sometimes, a limited availability of resources and support services further reduces people’s access to health services, increasing the likelihood of adverse health outcomes. For example, a shortage of doctors and primary care providers may mean patients wait longer to receive care.
Unreliable or inconvenient transportation can also make it difficult for people to receive consistent healthcare, potentially contributing to adverse health outcomes.
4. Neighborhood and Built Environment
The neighborhoods and built environments in which people live, work, play and learn can strongly influence their health and well-being for better or worse, depending on the circumstances.
Many people live in communities or work in jobs that present health risks like high rates of violence, pollution, unsafe water and others. Minorities and low-income people are more likely to live in neighborhoods and work in environments that present these risks.
The factors that make neighborhoods and built environments a social determinant of health fall into the following four groups.
Access to healthy foods: Access to nutritious foods is crucial to a sensible eating pattern. A lack of access to healthy foods can result in malnutrition, higher obesity levels and other diet-related conditions because low-income people tend to live in “food deserts.” However, accessing healthy food depends on more than having a grocery store nearby. People must also be able to afford it and affordability closely relates to employment rates and job quality.
Quality of housing: A home’s design and structure can significantly impact housing quality. Unsafe conditions such as the presence of asbestos, mold, lead, substandard air quality and overcrowding can lead to adverse physical and mental health outcomes.
Crime and violence: Whether experienced directly or indirectly, crime and violence can cause injury, mental distress and reduced quality of life. Some communities and groups are more likely to encounter crime and violence than others, such as low-income neighborhoods and Black adolescents.
Environmental conditions: Environmental conditions like water quality, air quality and the weather can influence a person’s health. Some groups are more vulnerable to poor environmental conditions and their associated health disparities. These include people of color, low-income families, the homeless, the elderly, pregnant women and children.
5. Social and Community Context
Social and community situations are vital aspects of a person’s health status. Relationships and interactions between people and their family, friends, colleagues and community can shape their health priorities and well-being.
Public health advocates classify social and community contexts into the following four categories.
Civic participation: Civic participation comprises activities like voting, volunteering, recreational sports, community gardening and more. Civic participation benefits the community and the participants by building social capital, expanding social networks and helping foster a sense of purpose.
Discrimination: Discrimination is a stressor that affects a person’s health by barring access to resources, dignity and quality of life.
Incarceration: People are more likely to develop chronic conditions like high blood pressure, cancer, asthma and arthritis. Black and Hispanic populations and people with low education levels have higher incarceration rates.
Social cohesion: Relationships are an essential part of physical and psychosocial wellness. Social cohesion is the strength of relationships and the perception of harmony within a community. High levels can positively influence health outcomes.
The Impact of Social Determinants of Health in Patients
Social determinants can dramatically impact physical and mental health outcomes, especially for vulnerable populations. Providers must account for circumstances like patient income, education and environment to deliver the holistic care necessary for health equity and well-being.
The public health sphere widely understands that poverty impedes access to nutritious foods and safe neighborhoods, and that higher educational levels contribute to better overall health.
If means are available to overcome adverse social determinants of health, populations can experience better health. But without resources, social determinants can foster troublesome circumstances like discrimination and disparities. Moreover, undesirable social health determinants can affect a person’s knowledge of healthcare and resources and restrict access to them.
The Truth About Negative Social Determinants of Health
Children of adults who did not earn a high school diploma are more likely to grow up in areas with barriers to healthcare and health topics.
As income levels decrease, the risk of premature death increases.
There is a direct connection between lower income, smoking and shorter life expectancy.
Poor white people are less likely to live in neighborhoods of concentrated poverty.
A person’s living environment may influence that of future generations.
Disparity-related stress relates to health and is often the result of overlapping factors.
Stress harms children and adults throughout their lives. Repeated exposure to environmental and social stressors may result in a cumulative burden that puts people’s health at risk.
Social determinants that result in health disparities are expensive and can hinder the quality of care that people receive, leading to additional healthcare expenditures, loss of efficiency and early death.
Research related to the price of health disparities puts the situation into perspective. For Black people, Hispanics and Asian Americans, 30% of direct medical costs relate to health inequities. On a broader scale, the U.S. loses approximately $309 billion each year to the direct and indirect costs of health disparities.
How ProspHire Can Help You Provide Quality Patient Care
As our population diversifies, it becomes more vulnerable to the concerns associated with adverse social determinants of health. One straightforward path to addressing this issue is coordinating services across the spectrum of care. Merging social support and assistance with healthcare delivery is vital for providers to confront the various social determinants that have such a bearing on patients’ wellness.
ProspHire prioritizes helping you provide high-quality healthcare to your patients, and we tailor solutions to do that. We understand the far-reaching effects that nonmedical factors have on a person’s health, so we’ve implemented strategies to help healthcare professionals address them.
Below are the services we offer related to social determinants of health.
SDoH solutions: These solutions allow you to look beyond the point of care and address all areas that impact health outcomes, such as housing, food insecurity, transportation and improving access to needed community programs.
Population health assessment and transformation: Assess your population, understand the underlying drivers of health and implement change to address social determinants and equitable health outcomes through turnkey interventions.
Organizational strategic planning: Drive organizational transformation through defined goals and a developed playbook for change management and actionable strategies to address health disparities.
Community-based partnership development: Evaluate, align and partner with community-based organizations to address social determinants and close care gaps to improve equitable outcomes and increase community-based care management.
Maternal health equity: Address inequities and improve outcomes in maternal health through population-based interventions and recommendations curated to meet the needs of vulnerable patients and members.
Quality accreditation achievement: Be a leader in the industry through the pursuit and award of health equity and other quality accreditations.
With these services, health providers can build a more comprehensive awareness of the biological, behavioral and social components that shape wellness and health systems. The result is an equitable healthcare system that makes better health outcomes attainable for everyone.
Address Social Determinants of Health with ProspHire
Tackling the challenges presented by negative social determinants of health is no small undertaking, but patients deserve your best effort. A multifaceted approach is necessary to make the changes that will allow our society to find health equity. ProspHire has the expertise and enthusiasm to develop a solid plan for your organization.
ProspHire helps our clients provide better access to quality healthcare. We’re here to help you implement the strategies and interventions needed to fight health disparities and achieve health equity.
With our commitment to culture, leadership, diversity, equity and inclusion, our minority-owned business is a leader in healthcare strategy and execution. Contact the experts at ProspHire today to learn more.
Social determinants, or drivers, of health (SDOH) were brought to the forefront of healthcare news during the COVID-19 pandemic. The virus disproportionately affected individuals with lower socioeconomic status and certain racial backgrounds, with the largest impact observed within inner-city, low-income housing across the United States. Healthcare experts believe that SDOH can account for as much as 90% of health outcomes, highlighting the need to address SDOH in our communities and innovatively reimagine care delivery.
Let’s Reimagine Care Delivery Through Pharmacies
The pandemic was a catalyst for pharmacists to participate in patient-facing care on a global stage. Members of the profession were able to provide COVID-19 test administration, vaccinations and patient education surrounding the virus. Pharmacies did not close their doors during any phase of the pandemic, unlike other businesses and medical offices. Hospitals and retail pharmacies remained operational to provide access to healthcare information and life-sustaining medications while the rest of the world was on pause.
In a perfect world, pharmacists would be able to balance medication dispensing and clinical services optimization for all patients at their practice sites. Addressing SDOH would be effortlessly placed into current workflow without disruptions in essential responsibilities and retail chain mandated vaccination quotas. The reality of the situation is that community pharmacists, often working understaffed with limited support resources, rarely have the time to complete their basic responsibilities in each shift. Many pharmacists stay after their required shifts or arrive to work hours before the pharmacy opens to complete backlogged medication dispensing from the day prior. As the world’s most accessible healthcare providers, pharmacists are often tasked to assist with patient care gap closure. Fully adopting the role of SDOH envoys is not possible under the current community pharmacy operational model. However, pharmacists can be empowered to address aspects of SDOH related to medication compliance.
Consider Practical Pharmacy Impact
One domain that pharmacists have the potential to intervene and assist patients with SDOH is financial insecurity. Prescription medication prices continue to rise year over year, impacting decisions that patients must make regarding adherence to their medication regimens. Lack of adherence can lead to decreased quality of life and increased healthcare dollar spend due to emergency room visits and hospital admissions. Upon prescription receipt, pharmacists can review applicable insurance coverage and patient copay fees to evaluate the patient’s true out of pocket expense. Pharmacists are encouraged to work as part of the patient’s healthcare team and alert prescribers to high-cost medications. Less costly therapeutic alternatives can be suggested to alleviate patients’ concerns involving pharmaceutical cost while improving healthcare outcomes.
Another common social determinant that can affect patients during a pharmacy encounter is transportation. Many patients located within urban areas of the country lack access to dependable transportation or the means to pay for this service. Rural access patients could have distances too far to travel to pick up their prescriptions on a consistent basis. Pharmacists have the capacity to check refill histories on their patients to identify compliance gaps in the current workflow. If refill disparities exist, the pharmacy has several options to consider. The pharmacist could explore the service of mail order prescription refills via the patient’s prescription drug coverage provider. However, the community pharmacy location would lose revenue from outsourced prescription fills. Many retail pharmacies offer prescription home delivery services for their patients. This option would be beneficial to both the patient and pharmacy if the service exists within the practice. Pharmacies could consider reduced or eliminated delivery charges for identified patients to further ensure medication adherence.
Future Endeavors
In the traditional retail pharmacy business model, pharmacists could use the Accountable Health Communities (AHC) Model1 developed by CMS for patient screening. This model contains questions that pharmacists could use to identify SDOH issues across multiple areas, including food insecurity, housing instability, lack of access to transportation, assistance with utility bills and interpersonal safety. Outpatient provider offices have used this tool in practice with mixed success rates, largely due to a lack of dedicated staff support. Pharmacists are not traditionally compensated for cognitive services, as the practice does not charge a fee-for-service (FFS) to patients receiving clinical information. Additional staffing, compensation and private counseling space would be essential to a pharmacy’s success in conducting SDOH screenings.
Redefining the Role of a Pharmacist from Medication Dispenser to Health and Wellness Ambassador
The public perception of pharmacists’ role in healthcare is elevated above a dispensing role at this time. Pharmacists have demonstrated the ability to do more than fill prescription medications and provide recommendations for over the counter (OTC) medications. The profession has the chance to redefine its role and shift once again from practitioners behind the counter to healthcare and wellness ambassadors. Increased effort is required to effectively address SDOH for our patients and the healthcare system. Can pharmacists effectively become innovative leaders in SDOH? Developing strong communication and information exchange with patients and their providers coupled with appropriate staffing resources in the pharmacy would be vital for success. Pharmacists can be powerful healthcare resources for addressing existing healthcare gaps. A rework of the industry business model to prioritize patient care and wellbeing would be a win for the profession and the public.
How ProspHire Can Help
At ProspHire, we want to help you and your members receive the highest quality of care. Our team’s extensive healthcare industry knowledge and commitment to valuable results can help you and your team optimize strategies to enhance healthcare delivery. Aligning analysis, insights and implementation regarding Social Determinants of Health with ProspHire’s expert team can help you address patient care as a whole. Our team is ready to have a conversation with you and understand your challenges experienced with SDOH application. Connect with us today.
The Centers for Medicare and Medicaid Services (CMS) require Mandated Documents for Medicare and Medicaid Beneficiaries, which describe member benefits and provide clear and accurate explanations through standardized templates. Since requirements change annually, it’s important for payors to update these documents and relay them to plan beneficiaries to maintain compliance.
Learn more about CMS medical record documentation requirements with ProspHire.
Who Needs the Required CMS Documentation?
Any provider approved to offer Medicare- or Medicaid-sponsored plans to their beneficiaries must comply with CMS Mandated Documents.
If you are approved to offer Medicare Advantage plans, you must follow the directives of Medicare and share up-to-date CMS Mandated Documents with beneficiaries.
What Are the Required Documents for CMS?
While CMS Requirements may vary by plan type, there are generally two categories of required documentation for CMS — communications and marketing. If a document is classified as a communication, it provides information to current or prospective enrollees. Marketing materials might include intent and content intended to draw an enrollee’s attention to particular information.
Plans must submit all marketing documents and some communications to the Health Plan Management System (HPMS) for review. HPMS requires some documents to be submitted by particular dates, while others are considered file and use (F&U), meaning the plan can use the materials five days after submitting them to HPMS for review. If the review finds any discrepancies, the plan may be subject to compliance actions.
These documents include the following:
Annual Notice of Change (ANOC)
Plans must send beneficiaries an ANOC each year, usually in the fall and no later than September 30. This document will detail any changes in cost or coverage that will take effect in January of the following year and is considered F&U.
ANOC and EOC Errata
If there are errors in the ANOC or EOC, plans must provide this document to enrollees immediately after they receive CMS approval.
Comprehensive Medication Review Summary
If enrollees are in a plan’s Medication Therapy Management program, they should receive this document immediately following the comprehensive medication review (CMR) or within 14 days.
Coverage/Organization Determination, Discharge, Appeals and Grievance Notices
If an enrollee has filed an appeal or someone has filed an appeal on their behalf, plans must issue this form based on the relevant time frames.
Enrollment/Election Form/Request
Plans must provide enrollment documents on request, and these materials require an HMPS review.
Enrollment and Disenrollment Notices
Medicare has very specific requirements for enrollment and disenrollment notices. Plans can find specific information on these materials in the Medicare Managed Care Manual.
Evidence of Coverage (EOC)
In the fall, plans must also send an annual EOC document that explains what the plan will cover the following year and how much beneficiaries must pay. This document falls under F&U review requirements.
Excluded Provider Notice
Providers can be subject to penalties for using individuals or entities listed in the Office of the Inspector General’s List of Excluded Individuals/Entities. CMS also keeps a list of excluded entities on the preclusion list. If an enrollee uses a provider listed on one of these excluded provider lists, plans must present them with this notice.
Explanation of Benefits — Part C
When enrollees use a Part C benefit, plans need to provide these materials monthly or per claim with a quarterly summary.
Explanation of Benefits — Part D
When enrollees use their prescription drug benefit, often referred to as Part D, plans must provide this documentation to enrollees by the end of the month following the month when they used their benefits.
Formulary
Also known as a drug list, this communication lists the prescription drugs a plan covers. Plans must make these documents available to enrollees annually by October 15.
Low Income Subsidy (LIS) Notice
If potential enrollees are eligible for Extra Help, plans must provide this document before the enrollment effective date.
Low Income Subsidy (LIS) Rider
Plans must provide this document to current Extra Help enrollees each year by September 30.
Membership ID Cards
Plans must provide both hard and digital copies of ID cards to their enrollees within either 10 calendar days of enrollment or before the end of the month before their enrollment.
Mid-Year Change Notification to Enrollees
If there is a change to the plan rules, benefits or formulary, plans must provide notice of these changes 30 days in advance, unless otherwise stated by the specific CMS regulations.
Non-Renewal Notices
If enrollees are impacted by a non-renewal or service area reduction, plans must provide this notice 60-90 days before the end of the contract year, depending on the material.
Outbound Enrollment Verification
If the enrollee is using an agent or broker enrollment, plans must provide this outbound enrollment verification by hard copy, telephone or email within 15 calendar days of the enrollment request.
Part D Transition Letter
If a beneficiary receives a transition fill for a non-formulary prescription drug, plans must send this letter within three days of adjudication.
Before reaching the plan termination effective date, plans must provide this notice by hard copy and newspaper publication.
Pre-Enrollment Checklist
Plans should provide this document alongside the Summary of Benefits (SB) before enrollment, in the same format the SB is delivered.
Prescription Transfer Letter
If an enrollee’s Part D sponsor requests to fill a prescription at an alternate pharmacy than the one they currently use, plans must send this letter in a timely manner.
Provider Directory
All plan enrollees will receive a provider directory annually by October 15 for current enrollees, within 10 days of enrollment for new enrollees and within three days for current enrollees when requested.
Provider Termination Letter to Beneficiaries
If an enrollee’s provider is no longer part of the plan’s network, plans need to notify enrollees by hard copy via mail 30 days before the effective date.
Safe Disposal Information
At a minimum of once annually, plans need to distribute information on the safe disposal of prescription drugs that constitute controlled substances, including information on drug takeback sites in the enrollee’s community.
Scope of Appointment (SOA)
The SOA form provides enrollees with the opportunity to mark which products they want to discuss, and plans must provide this via signed hard or electronic copy or telephonic recording before the appointment.
Star Ratings Document
The Star Ratings document is generated from HPMS following a standard format. Plans must provide one to enrollees before enrollment and upload the document for HPMS review within 21 days of the updated information.
Summary of Benefits
Plans must provide the SB to all enrollees annually by October 15 and submit the document for HPMS review by that date.
Disclaimers
Plans must also include any relevant disclaimers in all CMS required documents for patients.
ProspHire Can Help With CMS Compliance
Complying with CMS document requirements often requires annual updates with the participation of various departments, which can impact an organization’s efficiency and optimization. However, failing to meet the document requirements for government programs like Medicare and Medicaid can lead to non-compliance actions like fines and member abrasion.
ProspHire can help organizations maintain compliance and streamline their required documentation delivery management systems. With resources like a Required Documents Playbook and Program Toolkit, ProspHire can help organizations create a foundational operating model to ensure plan beneficiaries receive the necessary documentation on time.
Contact us through the form below to learn how we can help optimize your required documentation processes.
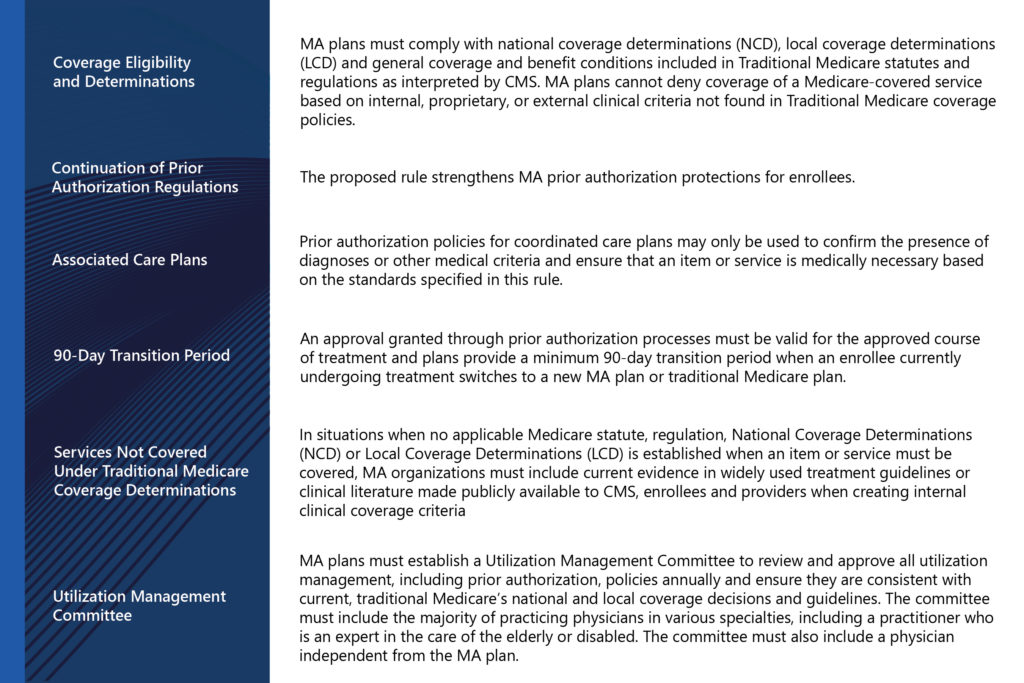
On December 14th, 2022, the Centers for Medicare & Medicaid Services (CMS) released proposed revised regulations governing Medicare Advantage (MA or Part C), the Medicare Prescription Drug Benefit (Part D), Medicare cost plans and Programs of All-Inclusive Care for the Elderly (PACE). The proposal’s focus is to increase transparency, improve health equity, reduce the cost of care and improve access to behavioral health services.
Key Medicare Advantage and Part D stakeholders will be able to provide feedback and analysis to CMS regarding the impact of these proposed changes by February 13, 2023. The proposed revisions would begin to take effect, offering guidance for the Medicare Advantage (MA) program contract year 2024.
Prior authorization can be used in a manner that results in potentially delayed patient care, burdens healthcare providers and adds unnecessary costs to the healthcare system. In summary, will focus primarily on the impact the proposed revised regulations have on utilization management and prior authorization. The effort to streamline the prior authorization process and promote healthcare is to improve the care experience across providers, patients, and caregivers.
The goal of the changes is that enrollees will receive the same access to medically necessary care they would receive in Traditional Medicare.
Key Points
What does this mean for MA plans?
For some plans, this legislative change means it is time to re-evaluate current policies and procedures in utilization management and ensure that current practices are consistent with the proposed rule. It is the time to review all existing policies and procedures related to prior authorizations, re-examine workflows and determine if staff have access and are using current traditional Medicare coverage determination materials. It is also time to establish if all coverage determination materials developed by the plan meet the requirements for development and communication. Consideration should also be given to the membership of the utilization review committee and determining if additional members are needed to cover the full scope of the specialties required to provide utilization review oversight.
How can ProspHire help
We know that a well-functioning utilization management process can improve costs, patient and provider satisfaction and compliance with regulatory requirements. With our experience in utilization review processes, policies, procedures and medical review, ProspHire can provide a baseline assessment, change management roadmap and assist with increasing efficiency, effectiveness and compliance in your utilization management functions. ProspHire focuses on best practices learned with plans across the country.
To connect with one of our experts, please fill out and submit the Contact Us Form.